
In 2019, the American Thoracic Society/Infectious Disease Society of America (ATS/IDSA) revised their guidelines towards the evaluation and management of Community Acquired Pneumonia (CAP). Regardless of the criticisms regarding the quality of evidence, there are quite a few recommendations I think are worth noting for my co-residents.
Evaluation
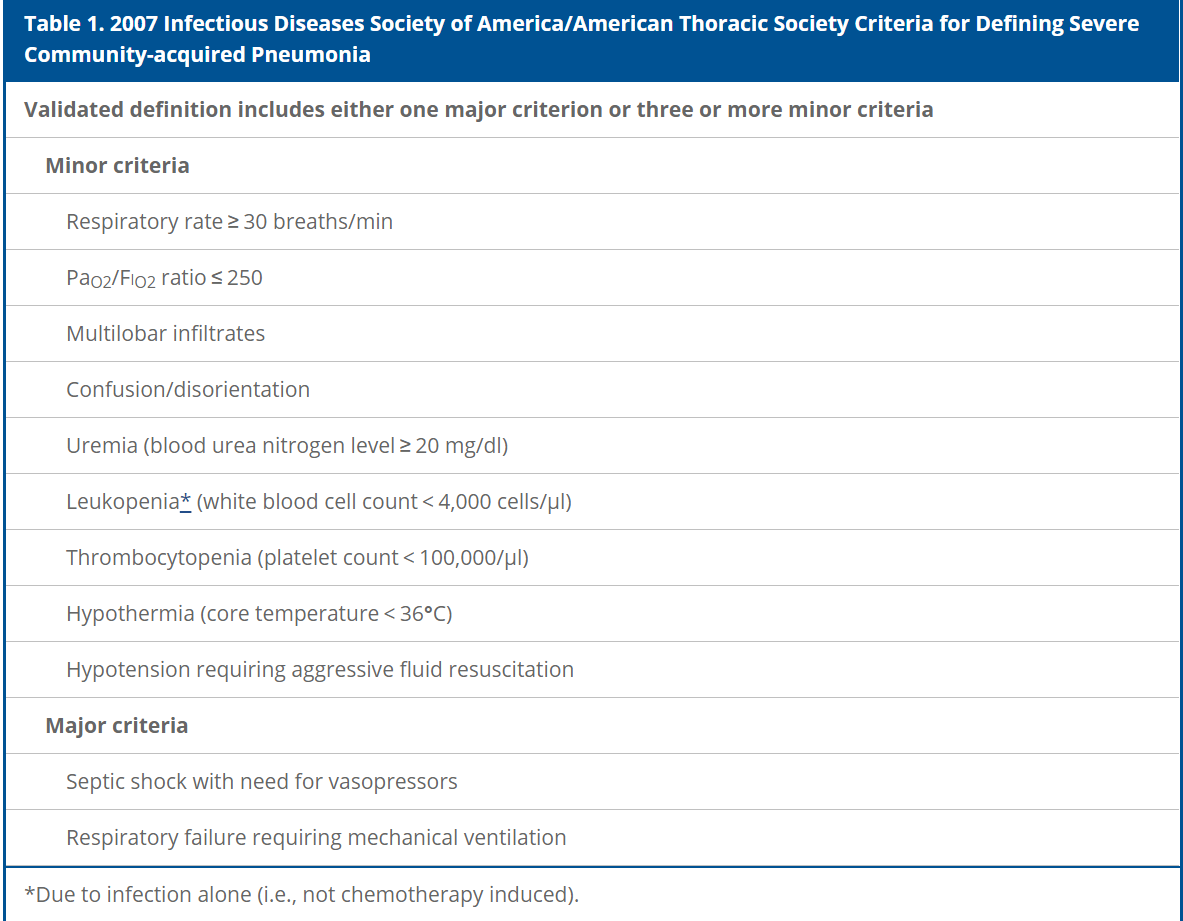
First, recall 2007 recommendations on classifying CAP as non-severe or severe
- Severe is 1 Major Criteria or ≥ 3 Minor Criteria
- Sputum and Blood Cultures? Obtain Sputum/Blood cultures ONLY in severe disease or history of MRSA/Pseudomonas
- Legionella Ag? Legionella testing only in Severe CAP or if known outbreak.
- Procalcitonin? Procalcitonin does not substitute clinical judgement in decision to treat even if Procalcitonin levels are low.
- Risk Stratification? Pneumonia Severity Index (PSI) is recommended over CURB-65 for prognostication.
The guidelines also revised their recommendations regarding treatment options. Given that most are tagged with a low or moderate quality of evidence, we as clinicians are obviously encouraged to use our clinical judgement by monitoring for clinical improvement and to use our hospital biograms.
Treatment | Inpatient
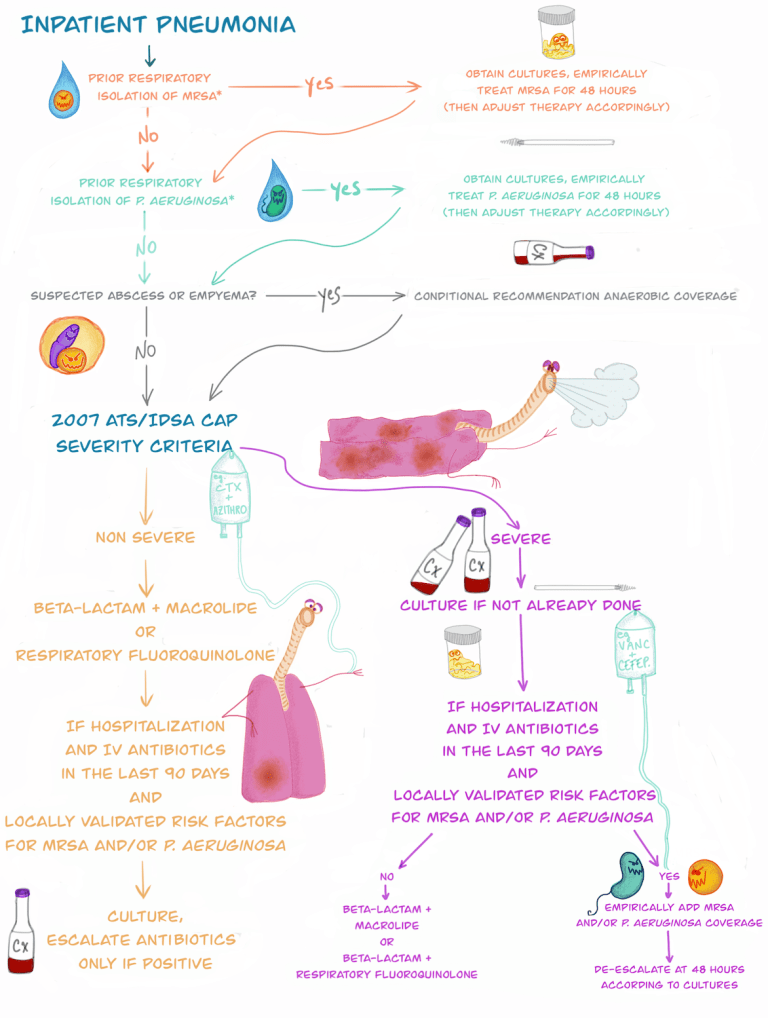
- Empirically treating patients with broad spectrum antibiotics (Vancomycin and Zosyn/Cefepime) just because of hospitalization within the past 90 days is no longer recommended.
- Non-Severe CAP with no MRSA/Pseudomonas risk factors
- Combo therapy: Beta-lactam + Macrolide
- Monotherapy: Respiratory Floroquinolone
- May use Beta-lactam + Doxycycline if contraindication to Macrolide or Quinolone
- Severe CAP with no/low suspicion for MRSA/Pseudomonas
- Combo therapy: Beta-lactam + Macrolide OR Beta-lactam + Floroquinolone
- Do not need to cover for Anaerobes unless concerns for lung abscess or empyema.
- Use Vancomycin for MRSA history or Zosyn or Cefepime for Pseudomonas history
- De-escalate MRSA/Pseudomonas coverage based on cultures.
- Steroids: not recommended.
- Treatment length of at least 5 days and patient achieving clinical stability.
Treatment | Outpatient
- No comorbidities: Amoxicillin 1g TID, Doxycycline 100 BID, or Azithromycin 250 daily (if local resistance to macrolides <25%)
- Comorbidities (CHF, Liver disease, Renal disease, Diabetes, EtOH, Cancer, Asplenia)
- Combo therapy with Augmentin 500/125 TID or 875/125 BID or Cephalosporin (Cefpodoxime 200mg BID or Cefuroxime 500mg BID) + Macrolide (or Doxycycline if contraindication to macrolide).
- Monotherapy with respiratory Floroquinolone
As a summary….
I’m a big fan of the history of medicine and it is interesting to see how these guidelines have changed.

References
- American Journal of Respiratory and Critical Care Medicine, Volume 200, Issue 7, 1 October 2019, Pages e45-e67, https://www.atsjournals.org/doi/full/10.1164/rccm.201908-1581ST
- PulmCCM, October 21, 2019. Jon-Emile S. Kenny. “2019 IDSA Guidelines for Community Acquired Pneumonia in Adults: To HCAP, we just say fare thee well.”
Post reviewed and edited by @udaygulati
