
You are reviewing your morning labs and the platelet count is awfully low. You start working through your differentials for thrombocytopenia and as you go through your list, you consider Heparin-induced thrombocytopenia (HIT). You glance over the medication administration record and there it is, your patient has been getting heparin. So should you be concerned about HIT?
Let’s review some HIT basics.
Mechanism
What are the types of HIT?
- Type I: Non-immune mediated transient decrease in platelets due to heparin. This is clinically insignificant.
- Type II: Immune-mediated HIT. This is what we care about.
What is the mechanism of type II HIT?
Courtesy of Laura Ibsen, MD.
- Heparin binds with platelet factor 4, resulting in an immune response where IgG antibodies form against heparin-PF4 complex.
- IgG induced platelet activation causes platelets to release their stored granules including more platelet factor 4 which recruits more platelets, resulting in a cascade of platelet aggregation and further activation and release of granules.
- Thrombocytopenia is a result of platelets being consumed in thrombi and from removal of IgG-coated platelets from circulation via splenic consumption.
- Note: It takes 5-10 days for plasma cells to make IgG Ab against hep-PF4.
Thus, the thrombocytopenia we see actually increases the risk of clotting, NOT bleeding.
Presentation
What is the clinical presentation?
- Thrombocytopenia +/- thrombus formation (can be either venous or arterial).
- Evaluate this with the 4T score (see below).
Which patients are at highest risk?
- Surgical patients receiving heparin (5% risk) > medical patients receiving heparin (~1%).
Does the type and dose of heparin matter?
- Type of heparin: Yes. The larger the heparin strand, the more likely it is to form a complex with PF4. Thus, the risk is higher with unfractionated heparin versus low-molecular weight heparin (80% lower risk versus UFH).
- Dose of heparin i.e. prophylactic versus therapeutic: No.
So how do we risk stratify patients?

What are the implications of the 4T score?
- Score of 6-8 = high risk
- Score of 4-5 = moderate risk
- Score <4 = low risk
So back to our main question, who to evaluate and treat?
- 4T score ≥ 4 indicates at least a moderate risk and these patients should have the two-step HIT workup initiated.
- *You must treat for HIT while the workup is pending (i.e. holding heparin alone is not enough)
- In our lab, we send out the HIT panel which includes both the optical density (“immunoassay”) and serotonin release assay (“functional assay”). These are sent out at the same time.
- The optical density immunoassay is the “screening test”.
- The serotonin release assay is considered “confirmatory.”
- In patients who are a moderate risk (4-5) and have a very LOW optical density score (< 0.6) rules out HIT.
- Otherwise, a very HIGH optical density (> 2.0) has a high likelihood of HIT and should continue to be treated.
In summary…
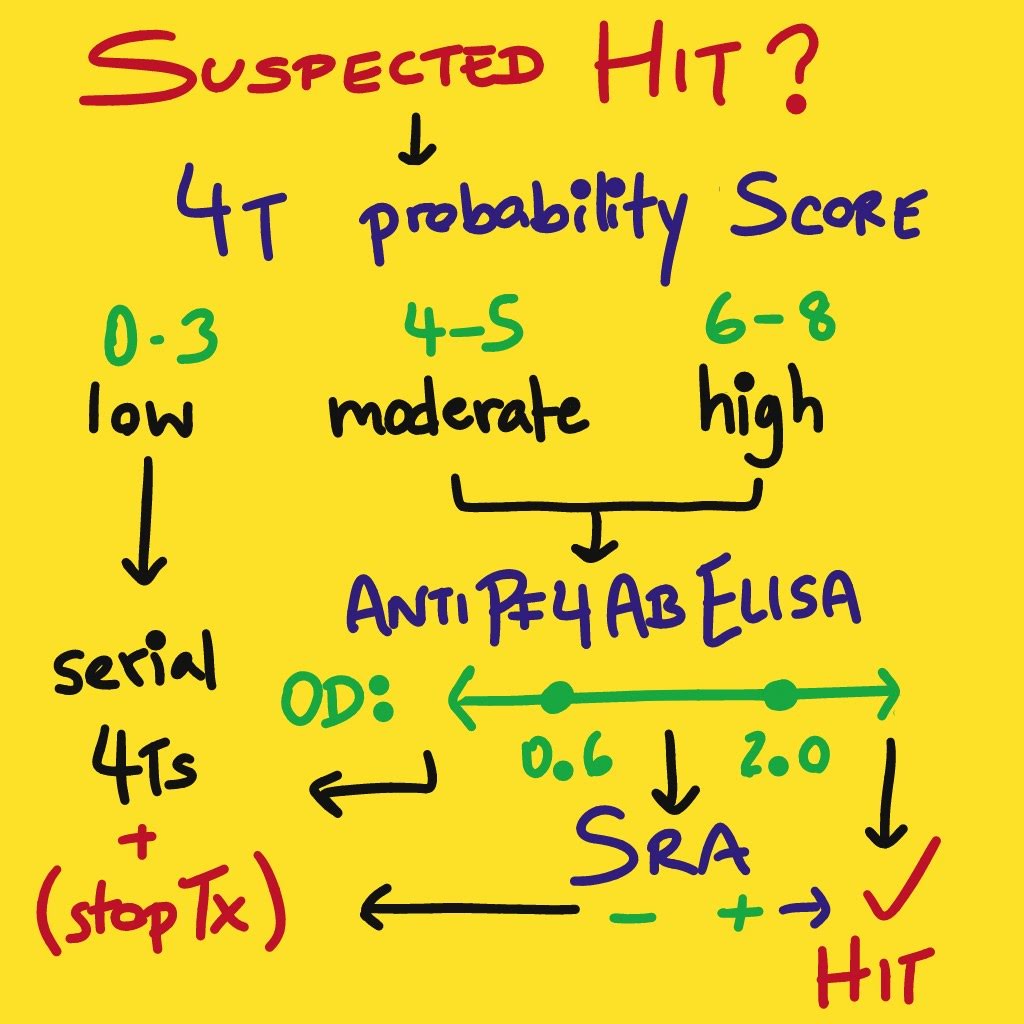
OD: Optical Density. SRA: Serotonin Release Assay
Drawn by @udaygulati.
So now you suspect or have confirmed HIT, how do you treat? Check out part II of this post.
References:
- Adam Cuker, Gowthami M. Arepally, Beng H. Chong, Douglas B. Cines, Andreas Greinacher, Yves Gruel, Lori A. Linkins, Stephen B. Rodner, Sixten Selleng, Theodore E. Warkentin, Ashleigh Wex, Reem A. Mustafa, Rebecca L. Morgan, Nancy Santesso; American Society of Hematology 2018 guidelines for management of venous thromboembolism: heparin-induced thrombocytopenia. Blood Adv 2018; 2 (22): 3360–3392. doi: https://doi.org/10.1182/bloodadvances.2018024489
- Coutre, S., & Crowther, M. (2020, January 2). Clinical presentation and diagnosis of heparin-induced thrombocytopenia. Retrieved from UpToDate
- Arepally GM. Heparin-induced thrombocytopenia. Blood. 2017;129(21):2864–2872. doi:10.1182/blood-2016-11-709873
- Linkins LA, Dans AL, Moores LK, et al. Treatment and prevention of heparin-induced thrombocytopenia: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines [published correction appears in Chest. 2015 Dec;148(6):1529]. Chest. 2012;141(2 Suppl):e495S–e530S. doi:10.1378/chest.11-2303
Post reviewed and edited by @udaygulati

One thought on “When are you concerned about HIT?”