
Before diving into the latest recommendations on antithrombotic therapy management of Peripheral Arterial Disease (PAD), a quick review:
Diagnosis of Lower Extremity PAD
- The vascular testing work up varies based on whether they are symptomatic or asymptomatic.
- For Asymptomatic, use a formal Ankle-Branchial Index (ABI) to confirm (more Sn/Sp than a bedside ABI for assessing location and severity)
- ABI ≤ 0.90 is diagnostic of PAD
- ABI 0.91 to 1.3 is normal and no further testing is indicated
- ABI > 1.3 should be followed with Doppler Ankle Waveforms and toe pressures (toe-brachial index, TBI) to rule out falsely elevated numbers from arterial calcifications in ESRD or DM patients
- For Symptomatic (claudication, rest pain, tissue loss, gangrene), usually more invasive testing is considered by our vascular surgery colleagues based on severity.

ABI: ankle brachial index; PAD: peripheral artery disease; MRA: magnetic resonance angiography; CTA: computed tomographic angiography.
Via UpToDate.
Risk Factor Modification
As internists, risk factor modification is the name of the game for patients with confirmed PAD. After all, it is a coronary heart disease equivalent. The goal of this post is solely focused on trying to simplify the antithrombotic therapy recommendations based on the latest literature, however understand that additional risk factor management for secondary prevention should include:
- Smoking Cessation
- Lipid Lowering therapy
- Glycemic control
- Antihypertensive therapy
- Diet and exercise.
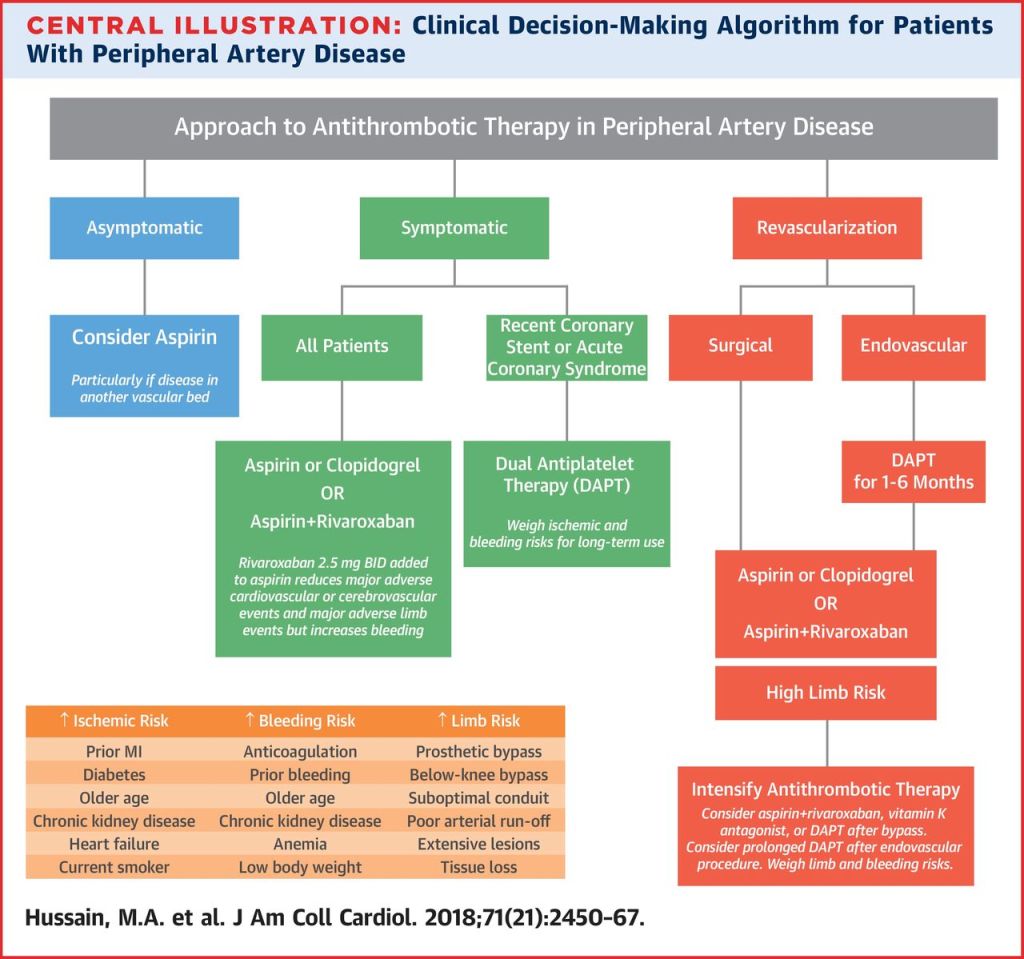
Antithrombotic Therapy
Just like with coronary artery disease, the recommendations regarding antithrombotic therapy have been extensively studied. Hopefully I can simplify the numerous recommendations based on the type of patient.
Asymptomatic PAD
- Consider use of Aspirin
- Evidence is mixed regarding use of Aspirin in this population however it is reasonable to start low-dose Aspirin.
- CLIPS Trial – Recommends low-dose Aspirin vs. POPADAD Trial – No benefit of Aspirin.
Symptomatic PAD
- Long-term single antiplatelet therapy (Aspirin OR Clopidogrel) is recommended.
- Clopidogrel is preferred over Aspirin (CAPRIE Trial)
- Dual antiplatelet therapy (DAPT) is NOT recommended unless other indications (e.g. drug-eluting stent) due to increased risk of bleeding.
- Warfarin + Aspirin was NOT more effective than Aspirin alone (WAVE Trial)
- Rivoroxaban alone has NO benefit compared to Aspirin alone (COMPASS Trial)
- Rivoroxaban + Aspirin has benefit over Aspirin alone but more bleeding (COMPASS Trial)
PAD s/p Revascularization
- Data is variable with no clear consensus regarding choice of therapy.
- DAPT with Aspirin + Plavix for 1-3 months followed by lifelong single antiplatelet agent.
- Clopidogrel is preferred (CAPRIE Trial)
- Aspirin + Warfarin can be considered in specific vascular situations (e.g. suboptimal conduit, compromised distal runoff, prosthetic graft)
- Rivoroxaban 2.5mg BID + Aspirin 100mg daily has shown benefit over Aspirin alone but has an increased bleeding risk (COMPASS Trial)
In Summary…
- Management of PAD should not be solely focused on antithrombic therapy but should also focus on risk factor modifications as listed above
- Ultimately choice of therapy is based on careful consideration of patient’s co-morbid diseases, risk vs benefit analysis, and shared decision making with the patient and their vascular surgeon.
References
Critical Leg Ischaemia Prevention Study (CLIPS) Group, Catalano M., Born G., Peto R. (2007) Prevention of serious vascular events by aspirin amongst patients with peripheral arterial disease: randomized, double-blind trial. J Intern Med 261:276–28
Belch J., MacCuish A., Camobell I., et al. (2008) The prevention of progression of arterial disease and diabetes (POPADAD) trial: factorial randomised placebo controlled trial of aspirin and antioxidants in patients with diabetes and asymptomatic peripheral arterial disease. BMJ 337:a1840
CAPRIE Steering Committee. (1996) A randomised, blinded, trial of clopidogrel versus aspirin in patients at risk of ischaemic events (CAPRIE). CAPRIE Steering Committee. Lancet 348:1329–1339
Warfarin Antiplatelet Vascular Evaluation Trial Investigators, Anand S., Yusuf S., et al. (2007) Oral anticoagulant and antiplatelet therapy and peripheral arterial disease. N Engl J Med 357:217–227Darmon A., Bhatt D.L., Elbez Y., et al. (2018) External applicability of the COMPASS trial: an analysis of the reduction of atherothrombosis for continued health (REACH) registry. Eur Heart J 39:750–757a.
Post reviewed and edited by @udaygulati
