
There are few oncologic emergencies that require an understanding of management at your fingertips. The approach to antibiotics for neutropenic fever is relatively simple so let’s review, starting with some basics.
DEFINITIONS
What is defines ‘Fever’ and ‘Neutropenia’ in Neutropenic Fever?
- Fever ≥ 38.3 or ≥ 38 sustained over 1 hour period.
- Avoid axillary temperatures as they may not be accurate.
- Rectal temperatures are avoided to prevent gut organisms form entering through mucosal surfaces.
- Neutropenia with fever is primarily concerning when it is severe: ANC < 500 or ANC expected to be <500 in 48 hours
- Mild: 1000-1500
- Moderate: 500-1000
- Severe: <500
What diagnostic tests should be performed in everyone with febrile neutropenia?
- CBC w/ differential, BMP, LFT’s w/ bilirubin (Evidence A)
- At least two sets of blood cultures from separate venipuncture (Two lumens if CVC in place or different peripheral sites) (Evidence A)
- CXR if respiratory symptoms present (Evidence A)
- Obtain Culture from other sites if suspected infection (For example: Lines, Catheters) (Evidence A)
RISK STRATIFICATION
How do you risk stratify patients with fever and neutropenia?
This index available on MDCalc helps risk stratify patients who are at low risk for poor outcome with febrile neutropenia. In fact, the score has also been endorsed by the Infectious Disease Society of America (IDSA) with Level B (moderate) evidence supporting its use. In simple terms, it classifies patients into low or high risk with the following:
| LOW Risk | HIGH Risk |
| • ≤7 days duration • no comorbidities ex. COPD | • > 7 day duration • prolonged neutropenia ≤100/mm3 • significant risk factors including hypotension, PNA, new onset abdominal pain or neurological changes |
TREATMENT
How do you act on the MASCC Risk Index score?
- MASCC < 21: High Risk
- Inpatient admission for treatment (Evidence B)
- MASCC ≥ 21: Low risk
- Outpatient management for treatment (Evidence B)
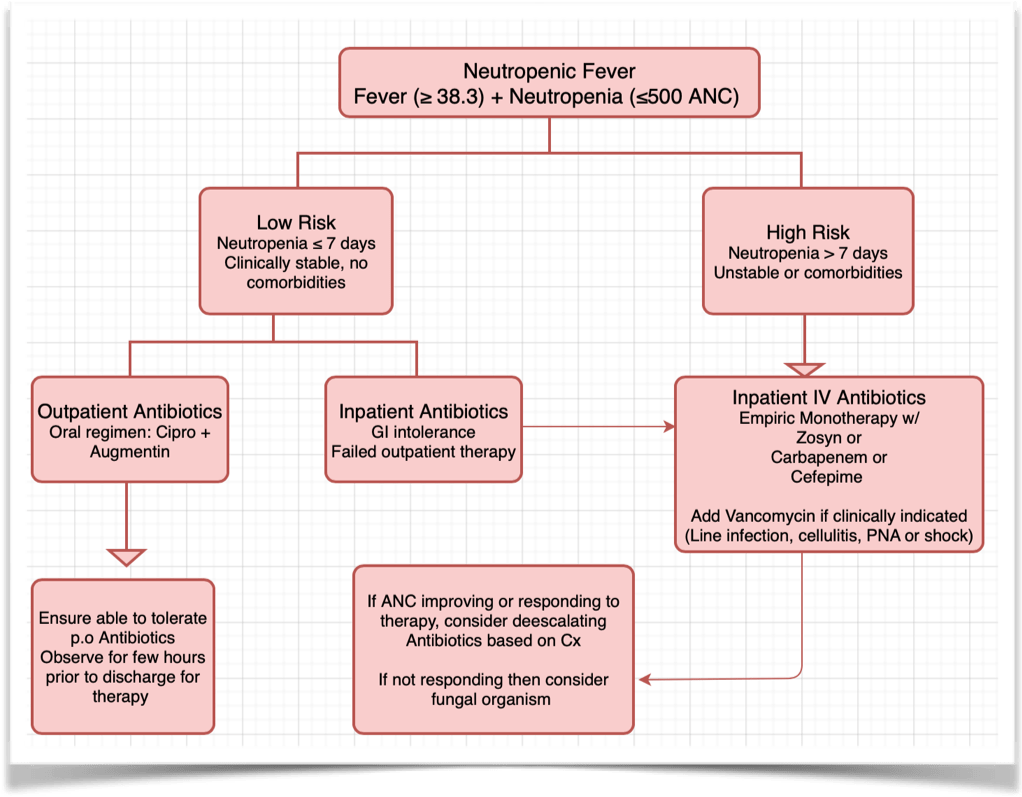
What therapy should be initiated in patients with fever and neutropenia?
You manage severe febrile neutropenia (ANC < 500 or expected drop), especially those with cancer, like you do sepsis. Initiation of antibiotic administration is time sensitive. In simple terms…
More specifically…
- High risk
- Anti-psuedomonal beta-lactam agent with cefepime, carbenepem, Zosyn (Any one) (Evidence A)
- Vancomycin may be added if complications or if resistance (Evidence B)
- Vancomycin if catheter related infection, skin or soft tissue infection, PNA or HD instability/shock
- If patient has a history of resistance to any of the following organisms:
- MRSA: Vancomycin, linezolid or daptomycin (Evidence B)
- VRE: Linezolid or Daptomycin (Evidence B)
- ESBL’s: Carbenepenem Evidence B)
- Penicillin allergy: Ciprofloxacin + Clindamycin or Aztreonam + Vancomycin (Evidence A)
- Low risk
- Ciprofloxacin + Amoxicillin-Clavulanate for outpatient therapy (Evidence A)
How long do you treat with antibiotics?
In simple terms: You treat until the ANC ≥ 500 (Evidence B)
More specifically:
- High Risk:
- If an infectious source of fever is identified, antibiotics are continued for at least the standard duration indicated for the specific identified infection (eg, 14 days for E. coli bacteremia)
- If no infectious source is identified then until afebrile ≥2 days and ANC ≥500 or showing increasing trend
- Low Risk:
- recovery of ANC ≥500
When should antifungal prophylaxis be considered?
- If there is no improvement in neutropenia after 48-72 hours.
- Prophylaxis should be provided/considered against Candida. Drugs such as Fluconazole, Voriconazole, or Capsofungin can be added.
- Prophylaxis for Aspergillus infection in transplant patients is not beneficial.
In summary…
- Early recognition of neutropenic fever, risk stratification, blood cultures and initiation of antibiotics with pseudomonas coverage is necessary.
- Consider Additional coverage with vancomycin if indicated or fungal coverage if resistance/no improvement.
References
Clinical Practice Guideline for the Use of Antimicrobial Agents in Neutropenic Patients with Cancer: 2010 Update by the Infectious Diseases Society of America
Clinical Infectious Diseases, Volume 52, Issue 4, 15 February 2011, Pages e56–e93
Carratala J, Roson B, Fernandez-Sevilla A, et al. Bacteremic pneumonia in and neutropenic patients with cancer: causes, empirical antibiotic therapy, and outcome, Arch Intern Med, 1998, vol. 158 (pg. 868-72)
Hughes WT, Armstrong D, Bodey GP, et al. 2002 guidelines for the use of antimicrobial agents in neutropenic patients with cancer, Clin Infect Dis, 2002, vol. 34 (pg. 730-51)
Post reviewed and edited by @udaygulati

Strong work #dvtppx
LikeLike