
A 42 year old female without history of cirrhosis or renal impairment presents with fatigue and slight yellowing of her skin. She denies any weight loss and shows no evidence of blood loss. Her labs show normocytic anemic with an elevated indirect bilirubin. Otherwise, her comprehensive metabolic panel is relatively unremarkable.
Weakness. Jaundice. Anemia. Indirect Hyperbilirubinemia. All signs point to sequela of hemolytic anemia. Lets investigate further.

When should we suspect hemolytic anemia?
Patients with hemolytic anemia typically present with the classic symptoms of anemia such as fatigue, lightheadedness, and/or dyspnea on exertion. In more pronounced cases, patients may experience tachycardia or orthostatic hypotension. The MCV is usually normocytic. What distinguishes hemolytic anemia from other forms of anemia are the presence of jaundice or dark urine, however these are not always present. Hemolytic anemia should be considered in any patient with anemia lacking evidence of blood loss.
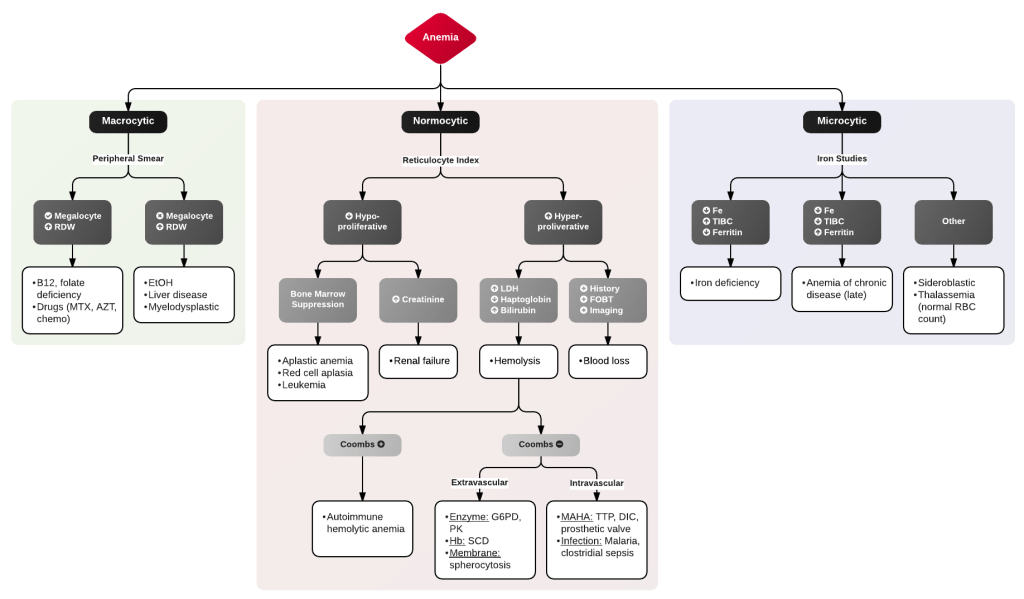
Another approach is work through your anemia algorithm. There are many out there, check out this straightforward one on ddxof.com.
What are the differentials for hemolytic anemia?
Differentials for hemolysis are extensive and can be categorized in numerous ways. These include:
| Intrinsic | vs | Extrinsic |
| Inherited | vs | Acquired |
| Acute | vs | Chronic |
| Immune destruction (due to antibodies) | vs | Non-immune destruction |
| Intravascular (in the vasculature) | vs | Extravascular (reticuloendothelial macrophages in liver and spleen) |
In going with the intravascular versus extravascular categories check out this simple table reproduced by @udaygulati from UpToDate.

Where should our workup begin?
Reticulocyte count: usually one would order this with every normocytic anemia without active bleeding. Reticulocytes are immature RBC’s that circulate in the bloodstream for about two days before they mature into RBC’s. Once obtained, be sure to calculate the corrected Reticulocyte Count which is then used to calculate a Reticulocyte Production Index (RPI).
Corrected Retic Count = %retic x Hct/45
Equation for corrected reticulocyte count. 45 represents the usual normal Hct.
RPI = Corrected Retic Count / RMT
Equation for Reticulocyte Production Index (RPI). RMT or the reticulocyte maturation time, usually 2, represents the maturation time correction factor as it takes most reticulocytes about 2 days before they mature into RBCs.
- An elevated RPI (>2) is a physiological response usually due to hemolysis or hemorrhage.
- A decreased RPI (<2) suggests normal or impaired RBC production.
- Note: some sources may use 2.5 suggest using >/< 2.5 instead of 2.
Why might the reticulocyte count be falsely normal?
Obtaining the reticuloycte count too early in the disease process or bone marrow pathology/intramedullary hemolysis may result in the reticulocyte count being normal. While checking the reticulocytes may be a good starting point, there are additional findings that can confirm your suspicion for hemolysis.
What other labs may be helpful?
Let us break it down by the commonly drawn labs:
Iron Panel: Total iron, TIBC, % iron saturation, and ferritin are usually normal.
“Hemolysis Labs”:
- Indirect Bilirubin is often elevated.
- LDH is often elevated.
- Haptoglobin is often decreased.
- Urinalysis may show hemoglobinuria.
Keep in mind that haptoglobin is also an acute phase reactant so it may be normal or high due to other processes. However, a haptoglobin level <25 is generally accepted to be indicative of hemolysis.
Peripheral blood smear: (labeled as ‘Doctor Smear’ on our EMR). If lucky, a look under the microscope can show notable abnormalities to help narrow the diagnosis.
Class pathognomonic findings to know include:
| Schistocytes | MAHA via mechanical shearing: TTP, HUS, DIC Mechanical heart valves |
| Spherocytes | Hereditary spherocytosis AIHA possibly extravascular hemolysis. |
| Elliptocytes | Hereditary elliptocytosis possibly myelodysplasia |
| Sickle cells | Sickle cell disease |
| Bite cells | G6PD Deficiency (look for unbitten Heinz bodies) |
| Intracellular organisms | Babesiosis (Maltese cross), Malaria |
| Ghost cells | Clostridial species |
| Teardrop cells | Bone marrow involvement |
Of note, because extravascular hemolysis is caused by phagocytosis of RBC’s by macrophages in the spleen and liver, the usual hemolysis labs above may not be positive. Some causes include RBC membrane abnormalities (ex. due to bound immunoglobulins) or physical abnormalities (ex. sickle cells) that can lead to splenic sequestration. While spherocytes can sometimes be seen on peripheral blood smear, often the blood smear is normal.
Finally, we can use the Coomb’s test which is also known as Direct Antiglobulin test (DAT), which can help diagnose the Autoimmune Hemolytic Anemia (AIHA) conditions listed above. Classic associations to know:
| Direct Coombs | RBC antibodies or complement bound on the RBC |
| Indirect Coombs | plasma antibodies that can bind to RBC antigens |
| IgG | warm |
| IgM | cold |
In Summary..
- consider hemolytic anemia when you have anemia with indirect hyperbilirubinemia or normocytic anemia without bleeding
- calculate the reticulocyte production index and consider hemolysis if greater than 2 and no evidence of bleeding
- obtain additional lab tests to work through and narrow your hemolytic anemia differentials including hemolysis labs, Coomb’s testing and a peripheral smear
Management of certain etiologies of hemolytic anemia require immediate interventions, simultaneous to the workup. How do we manage these conditions? Follow-up with Hemolytic Anemia: PART 2! (Coming Soon!)
References
https://www.sciencedirect.com/topics/medicine-and-dentistry/reticulocyte-index
https://www.hopkinsmedicine.org/health/conditions-and-diseases/hemolytic-anemia
https://medlineplus.gov/ency/article/000571.htm
https://onlinelibrary.wiley.com/doi/epdf/10.1002/ajh.10062
https://synapse.koreamed.org/DOIx.php?id=10.3343/alm.2013.33.1.1
https://www.cmaj.ca/content/174/3/305.short
https://www.med-ed.virginia.edu/courses/path/innes/rcd/hemo.cfm
Post edited and reviewed by @udaygulati
