
A 72 y/o F being managed on the floor for sepsis due to a problematic urinary tract infection starts to complain of acute onset LUQ abdominal pain. She describes abdominal pain out of proportion to your physical exam, one that includes mild signs of distension without peritoneal signs. She now has occult blood in the stool. Aside from leukocytosis and an elevated lactic acid, her initial lab studies are unremarkable. You go through your GIB and abdominal pain diagnostic algorithms and immediately, you pause as you place “ischemic colitis” at the top of your differentials. How do you approach ischemic colitis? Lets review the basics.
What is the relevant anatomy?
Recall, ischemia in the colon occurs because of sudden, usually transient, reduction in blood flow to the colon. The arterial supply to the colon can be divided by branches of the superior and inferior mesenteric arteries (SMA, IMA).
| Ascending colon | SMA |
| Transverse colon | SMA |
| Descending colon | IMA |
| Sigmoid colon | IMA |
| Proximal rectum | IMA |
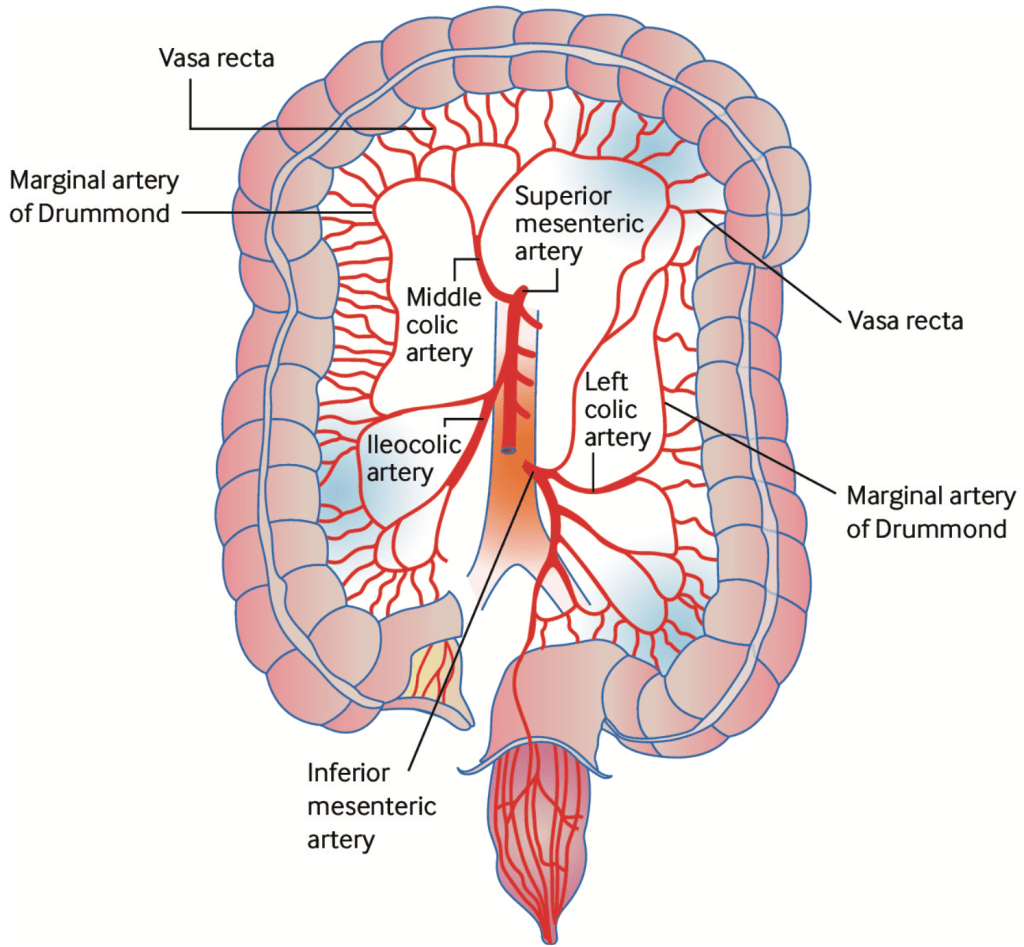
Most areas have a secondary collateral circulation that protects the large intestine from transient aras of inadequate perfusion. However, the areas between these collateral supplies, referred to as the watershed zones, are the areas that during low flow states will see the biggest decrease in blood supply. These are areas prone is ischemia. This is how the majority of cases of ischemic colitis occur.
| Splenic Flexure | between middle colic artery & left colic artery |
| Rectosigmoid Junction | between left colic artery & superior rectal artery |
What is the relevant pathophysiology?
Pathophysiology of compromised perfusion to the colon can be divided by three primary mechanisms:
| Nonocclusive | colonic ischemia caused by low blood flow ie the topic of this post |
| Occlusive | embolic or thrombotic arterial occlusion usually emboli from a proximal source |
| Venous | mesenteric venous thrombosis rare in the colon |
The decreased perfusion leads to hypoxia which leads to an ischemic event. Hypoxia initially leads to early mucosal injury and when prolonged, leads to irreversible full-thickness injury of the bowel wall. In these nonocclusive states, additional damage occurs following reperfusion or increased perfusion as limited blood flow is usually transient. This reperfusion leads to increased release of oxygen free radicals and eventually can lead to multisystem organ failure.
What are the risk factors?
This factors for intestinal ischemia include any condition that would compromise perfusion to the colon:
| Cardiac disease | · Cardiac emboli from arrhythmias, valvular disease, aneurysms · Low output into peripheral hypoperfusion, this includes any noncardiogenic hypovolemic state |
| Iatrogenic | · Aortic surgery or instrumentation that would dislodge intraluminal thrombus or atherosclerotic debris into intestinal circulation · Vasoconstrictive medications |
| Peripheral artery disease | Atherosclerotic occlusive disease of celiac artery, SMA, IMA |
| Hemodialysis | Causing low flow to intestinal circulation |
| Thrombotic conditions | 75% of mesenteric venous thromboses are due to inherited thrombotic disorders |
| Inflammation/infection | · Intestinal inflammation leading to venous thrombosis · Vasculitis predisposing to intestinal ischemia · Arterial infection leading to aneurysms which increases risk for thrombosis |
| Mechanical | Segmental ischemia from bowel strangulation from causes such as hernias, volvulus and over distention |
What is the usual presentation?
Usually, a good history and physical exam will spark suspicion for the initial differential. Symptoms include colicky abdominal pain, diarrhea and rectal bleeding. An easy mnemonic:
B – bleeding from lower GI tract
C – cramping
D – diarrhea
A useful ROS to cut in half your long list of differentials for GIB is painful v nonpainful. Ischemic colitis is almost always painful.
Exam will usually reveal tenderness and voluntary guarding over the affected segment of the colon. If peritonitis is present then you you should obviously be concerned about full-thickness ischemia or perforation.
Further categorizations of symptoms include differentiating acute v chronic.
Acute ischemia: more likely to occur in older patients, women, those with atherosclerosis or patients in shock. Acute ischemic colitis usually will present with left sided abdominal pain followed shortly by hematochezia. Progression will vary depending on the severity of ischemia and the amount of bowel involved. Mild disease can be self limiting, whereas severe disease can progress to shock and death.
Chronic ischemia: may present with episodes of recurrent pain, especially after meals (increased demand from bowel after a meal, bowel doesn’t get enough oxygen in watershed regions). With enough episodes, patients can progress to forming colonic strictures.
What is the difference between ischemic colitis and mesenteric ischemia?
A common misnomer. Mesenteric ischemia and ischemic colitis, while completely different disorders, are often mixed together and usually have different illness scripts and initial treatment algorithms.
| Mesenteric Ischemia | Ischemic colitis |
| Small bowel | Large bowel |
| Usually occlusive due to thromboemboli | Usually due to nonocclusive low flow states |
| Sudden onset | More gradual onset |
| Abd pain “out of proportion” | Moderate abd pain & tenderness, bloody diarrhea |
| Tx: urgent surgery | Tx: usually conservative, surgery occasionally considered |
What is the recommended diagnostic workup?
In simple terms: obtain an urgent CT abdomen pelvis with contrast and then a colonoscopy within 48 hours for confirmation.
Are abdominal x-ray imaging and ultrasonography useful? No. While often used they are not specific or sensitive enough though pathopneumonic both questions include thumbprinting on x-ray or mural thickening on ultrasonography.
Are lab tests useful? Sure. Usually the following markers will just increase your suspicion of something severe going on that requires urgent attention including elevated inflammatory markers (CRP, neutrophil count), decreased renal function due to an inflammatory response, elevated lactate. These are non-sensitive so normal markers does not exclude the diagnosis.
What am I looking for on the CT? These can diagnose ischemic let us and 98% of cases. Suggestive findings include wall thickening or abnormal enhancement, dilatation, venous engorgement, pneumatosis or portal venous gas, especially in the mentioned watershed regions.
When you get a CT angiogram? Reserve that for suspicion of mesenteric ischemia, not ischemic colitis. A CT abdomen pelvis with contrast will suffice. If you suspect an occlusive cause of ischemic colitis such as with isolated right colonic involvement (IRCI), consider the CTA.
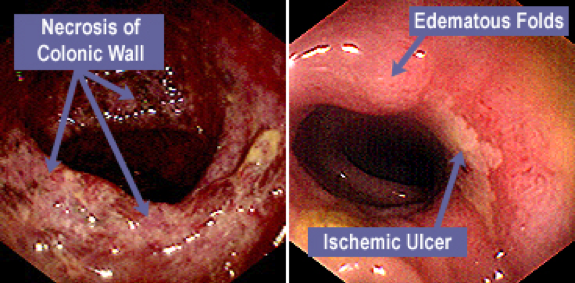
Why the urgent endoscopy? Confirmation and prognostication. The gastroenterologist will be looking for hemorrhages, edema, fragile mucosa, erosions and ulcerations, and sharply defined segments of involvement. Expect biopsies to be obtained.
What is the initial management?
ACG guidelines provide a neat initial management algorithm based on risk stratification. This will be done alongside your GI and surgical consultants.
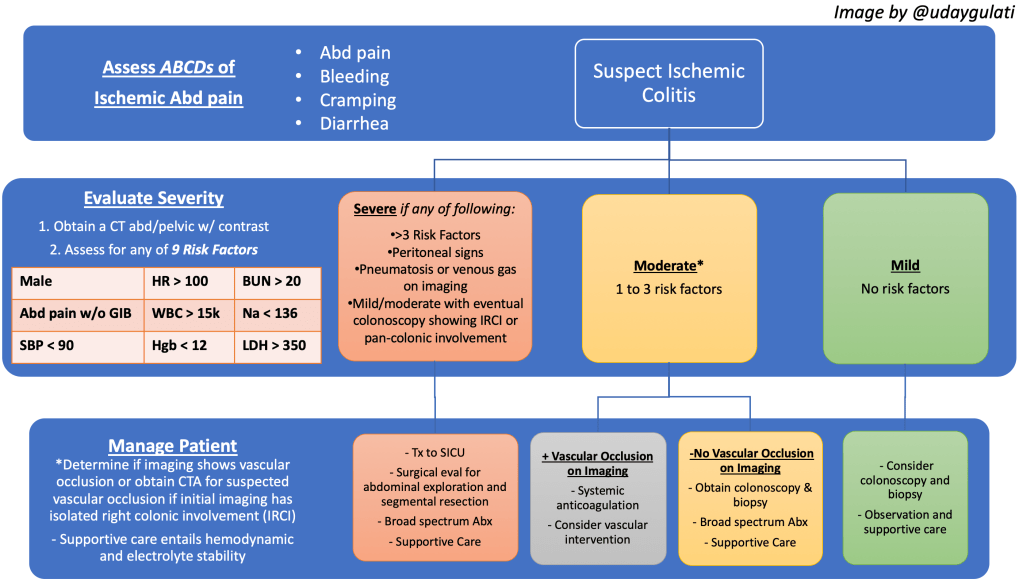
In summary, majority of cases are mild/moderate and to be managed with IV fluids and bowel rest. Patients require close monitoring with serial abdominal exams and labs to ensure no progression. Visible ulcerations on colonoscopy should prompt antibiotic coverage as these patients are at high risk for bacterial translocation into the bloodstream. A few more management pearls to keep in mind:
Do practice supportive care. That entails bowel rest, IV fluids to ensure adequate colonic perfusion, NG tube if ileus is present, discontinue precipitating meds and optimize cardiac function and oxygenation, especially if surgery is a possibility.
Consider opioids for pain control.
Consider systemic anticoagulation when suspecting thromboembolism or venous thrombosis and no contraindications i.e. bleeding or foreseeable operative management. An isolated right colonic involvement on imaging or colonoscopy raises suspicion for vascular occlusion. Otherwise provide usual prophylactic anticoagulation.
Consider surgery for perforation, generalized peritonitis and/or continuing hemorrhage. Discussed this further with the surgical weeks. Operative management can include segmental resection with colostomy formation.
Summary
- Ischemic small bowel? Mesenteric ischemia. Ischemic large bowel? Ischemic colitis.
- Ischemic colitis is typically acute in onset and requires urgent/emergent evaluation and management.
- Urgent evaluation means a stat CT with contrast and endoscopy within 48 hours.
- Urgent management means fluid resuscitation and antibiotics. Consider pain control. Consider anticoagulation.
References
Post reviewed and edited by @udaygulati
