
A 45-year-old male with history of hypertension presents to the emergency department complaining of abrupt onset dizziness that occurred when he stood from a seated position, the dizziness was accompanied by nausea and lightheadedness as well as a brief period of blacking out when the patient fell backward into his chair. He has never experienced this before. He reports increased physical activity on date of presentation because he is moving into a new apartment. Patient’s symptoms resolved spontaneously shortly after onset. Neurologic exam is negative. Physical examination is benign. ECG shows normal sinus rhythm with normal axis, normal interval and no ST-T wave changes. The patient is admitted to observation for workup of syncope. While it is common practice to obtain an echocardiogram, do you need it?
What causes syncope?
Simply stated, syncope is an abrupt, temporary loss of consciousness that occurs due to cerebral hypoperfusion with return to baseline function without intervention.
Below are some common causes of syncope, as adapted from Brignole, M. Heart 2007. The percentage of syncopal events secondary to arrhythmias or structural disease is generally less than 25%.

Figure 1. Brignole, M. Heart 2007;93:130–136. doi: 10.1136/hrt.2005.080713. Etiologies of syncope.
While a diagnosis of exclusion, in those with an unremarkable history, cardiac exam, ECG, CBC and BMP, majority of causes are vasovagal or orthostatic hypotension mediated.

What is the recommended evaluation of syncope?
Let’s begin with a few of the key points, relevant to our question, from the 2017 ACC/AHA/HRS Guidelines for the Evaluation and Management of Patients with Syncope.
1. Obtaining a thorough history and performing a good physical exam as well as an initial ECG in most beneficial in the initial diagnosis of syncope.
2. Identify the short- and long-term risk factors and use syncope risk scores to risk stratify patients ie do they need an additional workup? Do they need to be admitted to the hospital? The San Francisco Syncope Rule (https://www.mdcalc.com/san-francisco-syncope-rule) is the most well-known for ruling out high-risk syncope and helping to avoid unnecessary admissions.
- Other available scoring systems reported within the guidelines include OESIL (https://www.mdcalc.com/oesil-score-syncope) and the Boston Syncope Rule.
3. Hospital evaluation is only recommended for patients with serious medical history that could potentially be the cause of syncope. This includes arrhythmias that may require changes to medication, in the setting of long QT, or ICD placement, if VT noted. Also, cardiac causes – structural or valvular – requires treatment of the underlying condition. It is important to not forget about the larger noncardiac etiologies like severe anemia.
4. Routine cardiac imaging such as transthoracic echocardiography, CT or MRI do not provide any benefit unless a cardiac etiology, ie structural or an arrhythmia, is high on the differential.
So when do you get an echocardiogram?
Sarasin et al. published a study in 2002 is one of few studies that addresses the question we are posing – the utility of echocardiography in the evaluation of patient’s presenting with syncope. The study’s findings correlate with the 2017 guidelines. In a study including 155 people, they were able to determine that echocardiography is an important step in diagnosing patients with unexplained syncope with a positive cardiac history &/or abnormal ECG.
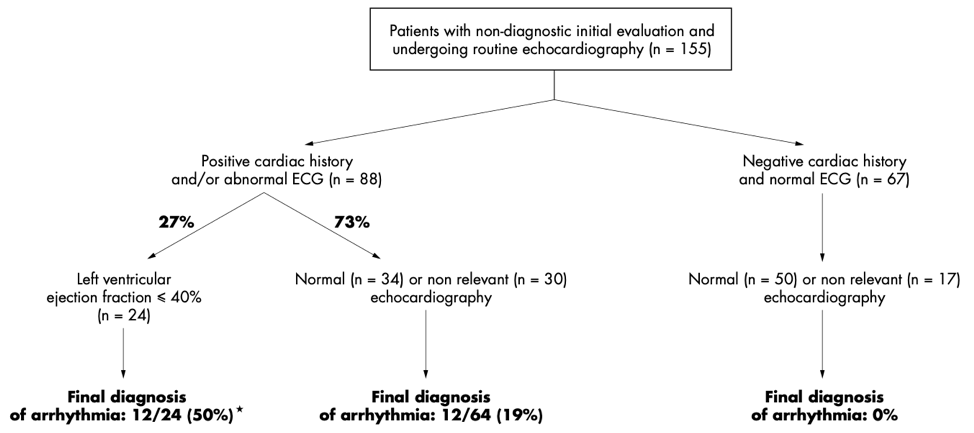
In patients with syncope that was not due to cardiac arrhythmia, as determined by the history, physical examination and ECG, echocardiography did not identify underlying disease. However, the evidence did show that echocardiography for patients who had concerning findings on initial evaluation identified disease and was useful in assessing the severity.
A more recent study aimed to assess the role of transthoracic echocardiography in evaluating patients who presented with syncope with a normal versus abnormal ECG. This study by Chang et al. in 2016 had 468 patients.
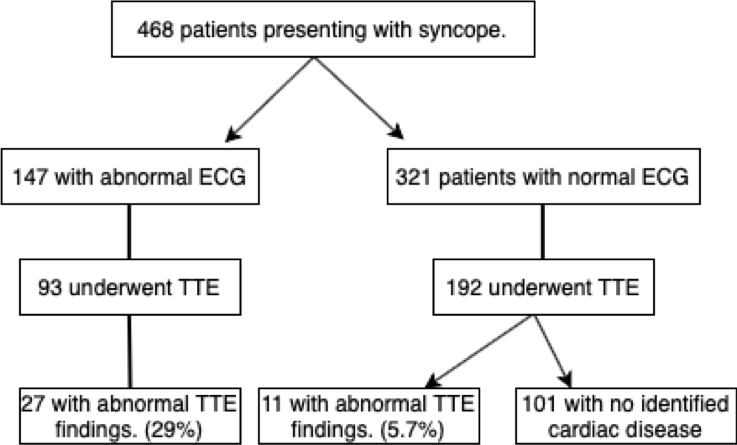
While there were ~6% of patients with positive TTE findings and per the study, some were known to have previously diagnosed AS on TTE, we are able to conclude that echocardiography is most useful in high-risk patients with cardiac history and/or EKG abnormalities. Maybe echocardiography should not be used routinely in patients presenting with syncope who do not meet the high-risk criteria. The above are two of many studies that have repeatedly recommended we follow the 2017 ACC/AHA/HRS guidelines regarding utilization of echocardiography in the evaluation of syncope.
Looking for a review of more studies? Need more evidence? Check out this great post on the Journal of Hospital Medicine’s blog Things We Do For No Reason: Echocardiogram in Unselected Patients with Syncope.
What are you looking for on an ECG?
What defines an abnormal ECG in syncope? Well, there is no set definition but per my literature review, important findings that should warrant further evaluation with an echo include:
| Bradycardia | Sinus Node Dysfunction 2nd/3rd degree heart block |
| Arrhythmias | PACs, PVCs Tachyarrhythmias (VF, VT, Afib, etc.) |
| QT changes | Prolonged QTc Shortened QT |
| Ischemic changes | STEs/STDs, T wave changes, Q waves |
| Miscellaneous | Bundle Branch or fascicular blocks WPW Brugada ARVD |
In summary…
- Obtain a thorough history and physical examination, including orthostatics and cardiac auscultation.
- Obtain an ECG. Interpret it. Look for the above.
- Risk stratify your patients using your clinical gestalt or a risk stratification score of your choosing before performing a TTE.
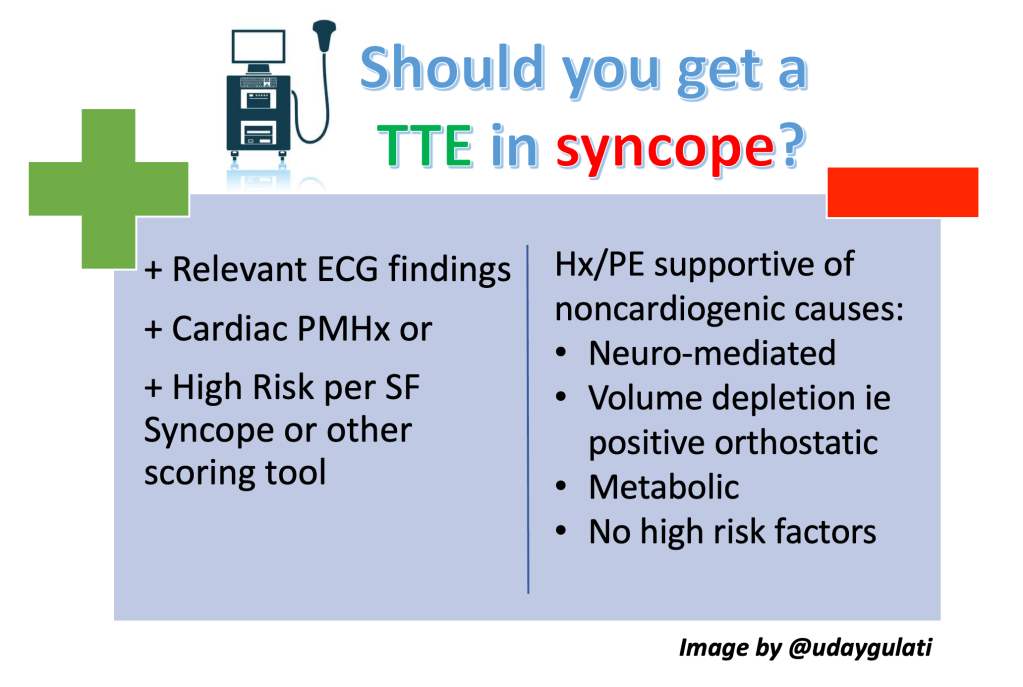
- Echocardiography is most beneficial in patients who have a concerning cardiac history, findings on examination or an abnormal ECG.
References
- Brignole, M. Diagnosis and treatment of syncope. Heart 2007;93:130–136. doi: 10.1136/hrt.2005.080713. Etiologies of syncope.
- Chang N et al. Diagnostic yield of echocardiography in syncope patients with normal ECG. Cardiology Research and Practice 2016. https://doi.org/10.1155/2016/1251637.
- Sarasin FP et al. Role of echocardiography in the evaluation of syncope: a prospective study. Heart 2002;83:363–367. doi: 10.1136/heart.88.4.363
- Shen WK et al. 2017 ACC/AHA/HRS Guideline for the Evaluation and Management of Patients with Syncope: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines, and the Heart Rhythm Society. J Am Col Cardiol. 2017; 70(5): e39-e110.
Post reviewed and edited by @udaygulati
