
On a recent post (When are you concerned about HIT?), we reviewed what you do when suspecting Heparin-induced thrombocytopenia (HIT). Recall, we talked about the mechanism, the clinical presentation, the risk factors, risk stratification and the workup. Pretty informative IMO. So as promised, here is part II, how do you treat HIT?
Who do you treat?
Recall, a 4T score ≥ 4 indicates at least a moderate risk and these patients should have the two-step HIT workup initiated. In addition, for these patients, you must initiate treat for HIT while the workup is pending (i.e. holding heparin alone is not enough).
As discussed previously and shown in the algorithm, you can stop treatment if the screening immunoassay is low (OD < 0.6) or the functional confirmatory assay is negative.
What is the treatment for HIT?
- Stop the heparin!
- you stop the heparin, you stop the platelet activation!
- this includes unfractioned heparin, LMWH, heparin flushes, heparin in catheters – DOCUMENT THIS WELL!
- there are rare forms of autoimmune HIT that result in continued platelet activation even with the absence of HIT – these require additional interventions beyond the scope of this post
- Start a non-heparin anticoagulant!
- Most of the time, the risk of thrombosis is higher than the risk of bleeding, even without evidence of a thrombotic event having already occured, that therapeutic-dose anticoagulation is required.
- A significantly low platelet count is not a contraindication to therapeutic dose anticoagulation in these patients.
Which non-heparin anticoagulant to pick?
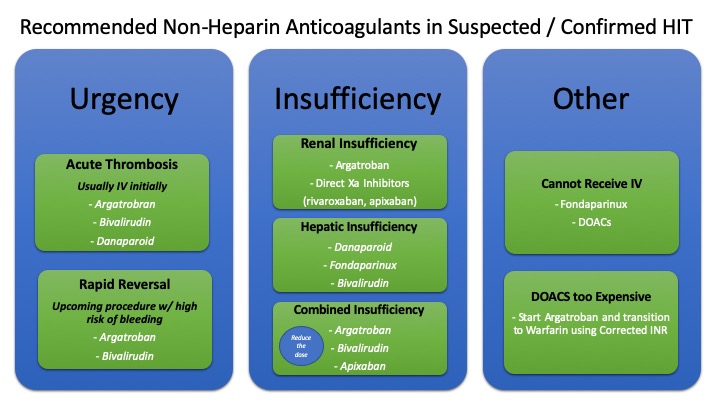
There are quite a few choices so picking one is based on several factors that include:
- urgency of need for anticoagulation
- consideration for need for rapid reversal
- renal and hepatic function
- cost
Options are plentiful and include Argatroban (infusion), Bivalirudin (infusion), Fondaparinux (Once daily SQ injection) or DOACs (PO, mainly Xarelto). UpToDate provides an extensive list of available options with a few pointers to consider with selection and a review of their mechanisms, administration and monitoring.
Can you use Warfarin to treat HIT?
Warfarin is contraindicated in acute HIT until platelets >150,000 because they are dependent on protein C to prevent thrombosis. Giving them Warfarin in acute HIT results in a hyper-coagulable state.
What is the duration fo treatment?
- If patient has HIT and thrombosis, then treat as a provoked clot (3 months)
- If patient has HIT and no thrombosis, then treat until platelet count recovers (>150, 000) plus a few additional weeks (generally 4-6 weeks)
| HIT w/ thrombosis | HIT w/o Thrombosis |
| Treat as provoked: 3 months | Treat until platelet count recovers (>150, 000) + a few additional weeks (generally 4-6 weeks) |
FAQs
I enjoyed this sign out because quite a few questions were brought up. As promised, here is what I found.
Do we screen patients that are stable and asymptomatic for clots if they have confirmed HIT?
Yes. They need bilateral LE duplex to rule out DVTs. If the patient has an upper extremity central venous catheter, they should get an upper extremity duplex as well. This is important because it is affects duration of treatment.
Do we transfuse platelets in patients with HIT?
No. Avoid platelet transfusions unless patient is actively bleeding out. Giving platelets in acute HIT is pro-thrombotic.
Do patients with confirmed HIT need IVC filters?
No. IVC filter is not recommended for these patients.
If your patient has confirmed HIT and needs to be anticoagulated for several weeks after discharge, but has no insurance, what do you send him home with?
- Start Argatroban in the acute phase and obtain daily PT/INR.
- The INR will be falsely elevated due to Argatroban so we need to calculate the corrected INR.
- You can use this formula to figure out when to discontinue the Argatroban and start Warfarin (assuming platelet counts are stabilized). Consultation with hematology is generally recommended.
Corrected INR = 0.19 + (0.57xINR)
Correction the INR while on Argatroban
Your patient has a history of remote HIT, what do you do for DVT prophylaxis while the patient is in the hospital?
Avoid heparin and low molecular weight heparin. You can go with: Fondaparinux, apixaban, rivaroxaban or VKA.
In Summary…
If you suspect HIT,
- Stop the Heparin!
- Start a non-heparin anti-coagulant. As discussed, there are quite a few non-heparin options.

Here is a quick breakdown when picking a non-heparin anticoagulant based on relevant considerations. Hope it helps!
References
- Adam Cuker, Gowthami M. Arepally, Beng H. Chong, Douglas B. Cines, Andreas Greinacher, Yves Gruel, Lori A. Linkins, Stephen B. Rodner, Sixten Selleng, Theodore E. Warkentin, Ashleigh Wex, Reem A. Mustafa, Rebecca L. Morgan, Nancy Santesso; American Society of Hematology 2018 guidelines for management of venous thromboembolism: heparin-induced thrombocytopenia. Blood Adv 2018; 2 (22): 3360–3392. doi: https://doi.org/10.1182/bloodadvances.2018024489
- Coutre, S., & Crowther, M. (2020, January 2). Clinical presentation and diagnosis of heparin-induced thrombocytopenia. Retrieved from UpToDate
- Arepally GM. Heparin-induced thrombocytopenia. Blood. 2017;129(21):2864–2872. doi:10.1182/blood-2016-11-709873
- Linkins LA, Dans AL, Moores LK, et al. Treatment and prevention of heparin-induced thrombocytopenia: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines [published correction appears in Chest. 2015 Dec;148(6):1529]. Chest. 2012;141(2 Suppl):e495S–e530S. doi:10.1378/chest.11-2303
Post reviewed and edited by @udaygulati

One thought on “How do you treat HIT?”