
The time has come. We have exhausted our resources. We have given our very best effort. We have decided that it is in our patient’s best interests to pursue the path of comfort rather than continued intervention. We are now faced with the question that many of us are undertrained and uncomfortable to answer:
how do we help our patients with the imminent dying process?
What is the Syndrome of Imminent Death?
As described by the Palliative Care Network of Wisconsin, author of Fast Facts, the syndrome of imminent death is a collection of symptoms that occur in the final hours to days of a patient’s life. There is a stereotypical pattern among dying patients and a general trajectory that each symptom represents. Duration of symptoms can last from about one day up to two weeks, and a patient’s baseline status has a significant influence on this (ie. Someone who is nutritionally intact vs. cachectic).
What are the stages of dying?
The Palliative Care Network of Wisconsin divides the dying process into three main stages, as follows. Recognizing these stages is important in order to guide management.
- Early: In the early stages of dying, patients will have decreased oral intake and may become delirious, spend more time sleeping, and become bed bound.
- Middle: As the patient progresses to the middle stage of the dying process, they may become increasingly obtunded and will be barely arousable.
- Late: Signs that your patient has entered the late stages of the dying process include coma, mottling of the skin, and changes in respiration pattern, including apnea.
What are the classic symptoms of Imminent Death?
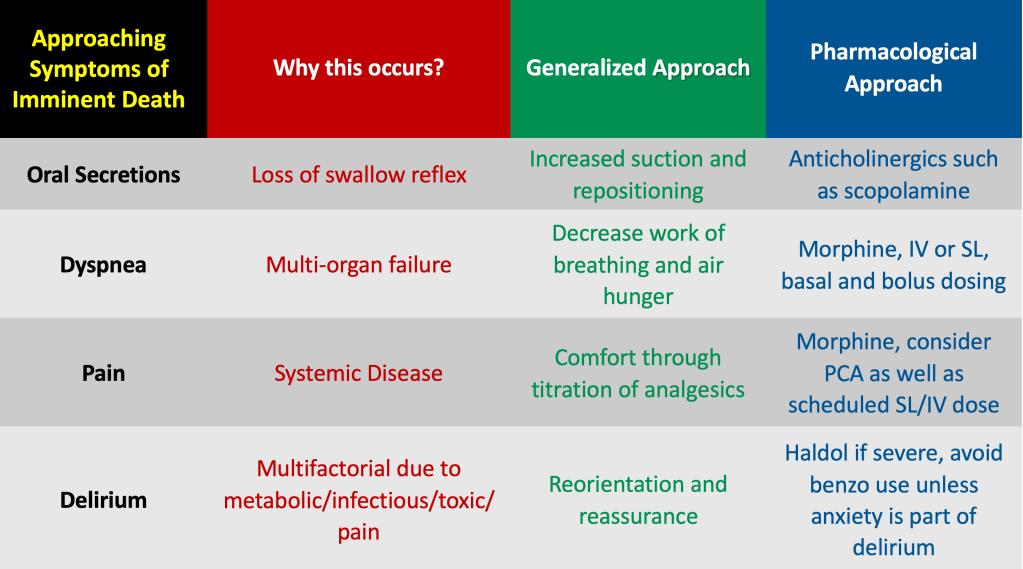
Although presentation and timing may vary, PCNW states that the four classic symptoms of imminent death are typically the same: increased oral secretions, delirium, pain, and dyspnea.
It should be no surprise that these symptoms are not only uncomfortable for the patient, but also difficult for the family and those at the bedside to experience. Part of your management should include helping the patient’s family to understand their loved one’s symptoms and what they should expect. For example, as the patient’s oral intake begins to decrease, the family may become concerned that the patient is “starving to death”. Gently explain to the family that the body requires less and less nutrition as the dying process progresses.
How do you approach the classic symptoms?
Let’s discuss some of the common symptoms and how to manage them.
- Oral secretions: Due to loss of swallowing reflex, dying patients will begin to pool secretions. This often leads to the rattling or gurgling sound described commonly as the “death rattle”. One study has indicated that the time of onset of the death rattle to death was only 16 hours. Although the increase in secretions cause no imminent threat to the patient themselves, it may be distressing to family members who feel the patient may be choking or “drowning”. Nonpharmacological treatment includes repeated suctioning and repositioning. Try an anti-cholinergic such as a scopolamine patch or sublingual hyoscyamine to reduce secretions.
- Delirium: The patient will become increasingly somnolent as the dying process progresses. Delirium may present initially with hallucinations, memory disturbances, and increased sleepiness. Family may express concerns of their loved one speaking with people who are not in the room or who are deceased. This is an exceedingly common phenomenon, and should be explained to family members as such. Treatment of terminal delirium should be mostly non-pharmacological, including help and support from family at bedside as well as reduction or increase in environmental stimulation as needed. Neuroleptics such as Haldol may be used, but should be considered second line. Benzodiazepines such as Ativan should be avoided, as they may worsen delirium, unless anxiety is the underlying cause of delirium.
- Dyspnea: Typically terminal dyspnea is caused by underlying multi-system organ failure, and is commonly the most distressing symptom to family. Classic management of terminal dyspnea is with opioids (classically morphine), which help to reduce air hunger through central respiratory depression. Initially, morphine may be administered a few times per day, but may be administered as frequently as every 5-10 minutes when symptoms become severe. A PCA dose may also be considered in an inpatient setting, which may be administered by a nurse, the patient, or family members depending on hospital policy. Otherwise, consider IV or SL dosing. Be prepared to discuss with family the concept of “hastening death” with opioids, although there is no data to show that management of terminal dyspnea has this effect. Discuss the benefits of symptom relief rather than the idea of “assisted suicide”.
- Pain: Luckily, morphine may be used to treat both dyspnea and pain, but careful consideration should be used when choosing a dose. Make sure to calculate an equianalgesic dose of the opioids that the patient is already taking. If this dose has not been effective, you can increase anywhere from 25-100%. This will be the patient’s basal dose, but a bolus or “rescue” dose should also be added. This may be done via IV, sublingual, or through use of a PCA. This dose (bolus) should be adjusted based on symptoms, which should be assessed every 15 minutes or so until desired effect is obtained. Obviously take into consideration the patient’s renal function as well as age to avoid the buildup of metabolites which may worsen delirium.
In Summary:
The dying process may vary by timing and severity of symptoms depending on the individual patient, but the common goal for providers should be to make this process as comfortable as possible for both the patient and his or her family.
In the interim, watch for the classic symptoms and consider managing them as below. As always, individualize and continue to evolve your approach for each patient.
References
Fast Facts, Palliative Care Network of Wisconsin.
Rousseau, P. Management of Symptoms in the Actively Dying Patient. Principles and Practice of Palliative Care and Supportive Oncology. 2nd Ed, 2002.
Signs of Impending Death. Stanford School of Medicine Palliative Care. https://palliative.stanford.edu/transition-to-death/signs-of-impending-death/
Post reviewed and edited by @udaygulati
