
You are on the wards taking care of a patient that was admitted for sepsis. The infectious source was unclear. He may have had a slight infiltrate suggesting a pneumonia. His urine was clean. His CT thorax and abdomen was unremarkable. After overall stability for two days, his initial blood cultures obtained in the ED come back positive for monomicrobial enterocci bacteremia.
How do you proceed?
Lets simplify an approach.
Why are enterococci clinically relevant?
Recall from early days of medical school, enterococci are gram positive cocci found in the GI tract and are clinically relevant due to being a relatively common cause of endocarditis, nosocomial urinary tract infections and bacteremia. In fact, enterococci, specifically, enterococci faecalis, are the third leading cause of endocarditis after Staphylococcus and Streptococci. They have also been reported to cause up to 15 to 20% of UTIs in hospitals. Unfortunately due to the many antimicrobial resistance mechanisms allowing these organisms to survive and proliferate when usual antibiotic susceptible organisms are eliminated, enterococci have become the second or third most common organisms in hospital acquired infections, with an increasing incidence of bloodstream infections, especially in those who are severely ill, have had prolonged hospitalizations or have receive multiple antibiotics. Enterococci have also been reported to cause meningitis.

The goal of this post is focused on managing monococcal enterococci bacteremia.
What are the potential sources of infection?
When evaluating monomicrobial enterococci bacteremia, the following portals of entry should immediately come to mind:
- the gastrointestinal tract,
- the urinary tract,
- intravascular catheters,
- and wounds (such as ulcers or burns).
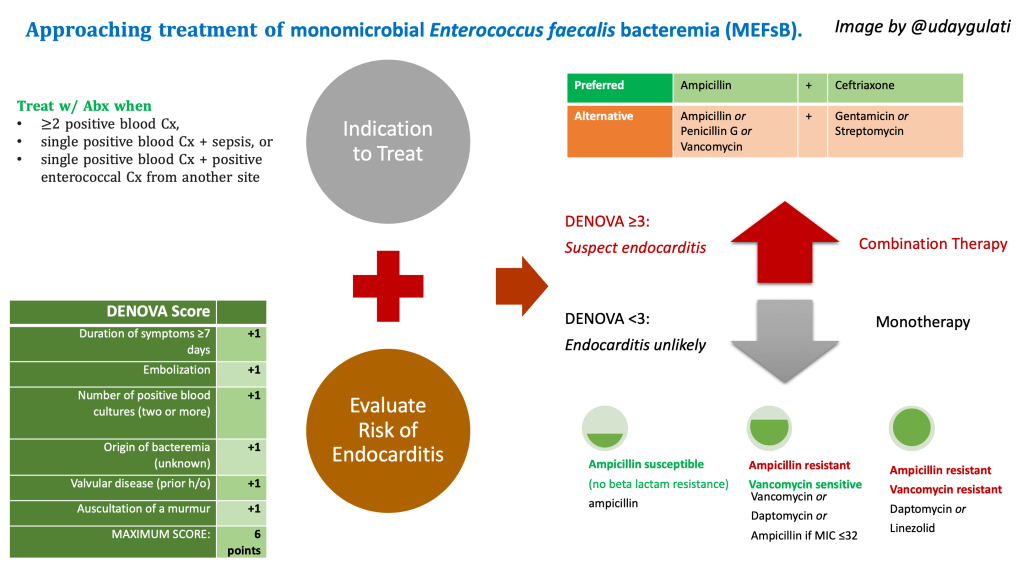
When do you consider antimicrobial therapy?
Generally, antibiotics therapy is warranted in any of the following scenarios:
- two or more positive blood cultures
- a single positive blood culture plus signs of sepsis, OR
- a single positive blood culture plus with positive enterococcal culture from another usual sterile site
Based on literature review and what seems like expert opinion, you can defer treating positive enterococcal bacteremia in those without a fever and
- who have only a single positive blood culture and are without any clinical evidence of sepsis,
- who have a polymicrobial infection and are improving on therapy for a more virulent organism,
- who are believed to have transmitted the infection from an intravascular catheter and have had the catheter removed.
When do you obtain an echo to rule out endocarditis?
As with many bloodstream infections, the feared complication of endocarditis needs to be considered. However, not everyone needs a workup with an echo! Most cases of enterococcal bacteremia due to species other than E. faecalis are not associated with endocarditis. And although the relatively risk of endocarditis is higher in such patients, it is still relatively low. To help assess the need for echocardiography evaluation, a clinical scoring system was developed: originally the NOVA score, since upgraded to the DENOVA score.
It may be a useful tool for prediction of endocarditis and the need for transesophageal echocardiogram (TEE) in those who have confirmed monomicrobial Enterococcus faecalis bacteremia (MEFsB). While not available on MDCalc, the mnemonic is pretty easy to remember:
| Duration of symptoms ≥7 days | +1 |
| Embolization | +1 |
| Number of positive blood cultures (two or more) | +1 |
| Origin of bacteremia (unknown) | +1 |
| Valvular disease (prior h/o) | +1 |
| Auscultation of a murmur | +1 |
| MAXIMUM SCORE: | 6 points |
A cutoff score of < 3 was associated with a low probability of IE, with a sensitivity and specificity of 100 percent and 85 percent, respectively.
In the Berge et al. trial testing this scoring system, the following parameters were used:
- Duration of symptoms: ≥7 days before the first positive blood culture was taken with any symptom compatible with IE
- Embolization: signs on clinical examination or by findings using imaging techniques (think Dukes minor criteria).
- Number of positive blood cultures: ≥2 or more blood cultures positive with enterococci faecalis and further classified as
- Community acquired: within the previous 90 days preceding an episode
- Nosocomial: blood culture drawn after 48 or more hours of hospitalization
- Origin of infection: focal infection w/ fulfillment of ≥2 of following:
- (a) typical signs or symptoms of infection
- (b) isolation of E. faecalis at the site of infection, and
- (c) imaging results compatible with focal infection which was likely to be the point of entry for the bacteria.
- Valve disease: history of any of the predisposing heart conditions that constitute a high or moderate risk of developing IE, including
- (1) native valve disease,
- (2) previous IE, or
- (3) the presence of a valve prosthesis
- Auscultation of murmur included those with any murmur reported
How do you treat monococcal bacteremia?
Without diving into too much detail, enterococci are relatively resistant to the killing effects of cell wall-active agents (penicillin, ampicillin, and vancomycin) and are impermeable to aminoglycosides.
For treatment of enterococcal bacteremia WITHOUT suspected endocarditis:
Susceptible enterococcal bacteremia: preferred monotherapy consists of Ampicillin. Alternatively, in the setting of beta-lactam resistance or true allergy,
Resistant enterococci bacteremia can further be categorized into
- ampicillin-resistant, vancomycin-susceptible: – Vancomycin or Daptomycin may be administered. High-dose ampicillin may be used if the ampicillin MIC is ≤32 mcg/mL.
- ampicillin- and vancomycin-resistant: Daptomycin (8 to 10 mg/kg/day) or linezolid (administered orally or intravenously) are reasonable therapeutic choices.
For treatment of enterococcal bacteremia WITH suspected endocarditis or critical illness, combination antimicrobial therapy is recommended over monotherapy (Grade 1B). Combination Ampicillin plus Ceftriaxone is preferred, since it avoids the toxicity of aminoglycosides (Grade 2B); however, use of a cell wall-active agent in combination with a synergistically active aminoglycoside is also acceptable. Specifically:
| Preferred | Ampicllin | + | Ceftriaxone |
| Alternative | Ampicillin or Penicillin G or Vancomycin | + | Gentamicin or Streptomycin |
How long do you treat?
Optimal duration of antimicrobial therapy remains uncertain.
For uncomplicated infection, five to seven days of therapy from the first day of negative blood cultures is likely adequate.
Treatment of infective endocarditis will vary based on the valve (native vs prosthetic) but generally ranges up to six weeks.
In Summary:
- consider sources of enterococci when positive on cultures
- Don’t treat everyone w/ a positive Cx. Treat w/ Abx when
- ≥2 positive blood Cx,
- single positive blood Cx + sepsis, or
- single positive blood Cx + positive enterococcal Cx from another site
- Obtain a TEE to rule out endocarditis when DENOVA score ≥ 3
- Follow the antimicrobial ladder as below to treat pending sensitivities
References
Beganovic M, Luther MK, Rice LB, et al. A Review of Combination Antimicrobial Therapy for Enterococcus faecalis Bloodstream Infections and Infective Endocarditis. Clin Infect Dis 2018; 67:303.
Berge A, Krantz A, Östlund H, et al. The DENOVA score efficiently identifies patients with monomicrobial Enterococcus faecalis bacteremia where echocardiography is not necessary. Infection 2019; 47:45.
Britt NS, Potter EM, Patel N, Steed ME. Comparative Effectiveness and Safety of Standard-, Medium-, and High-Dose Daptomycin Strategies for the Treatment of Vancomycin-Resistant Enterococcal Bacteremia Among Veterans Affairs Patients. Clin Infect Dis 2017; 64:605.
Graninger W, Ragette R. Nosocomial bacteremia due to Enterococcus faecalis without endocarditis. Clin Infect Dis 1992; 15:49.
Post reviewed and edited by @udaygulati
