
A 35-year-old male with history of asthma presents with new onset fever, fatigue and non-productive cough. Her symptoms and workup matched that of a COVID-19 illness script. After being admitted due to some level of respiratory distress and for close monitoring with appropriate airborne precautions, her COVID-19 PCR test comes back positive. You discuss with your colleagues and consultants the efficacy of current popular therapies.
How does the pathogenesis of SARS-CoV-2 relate to treatment options?
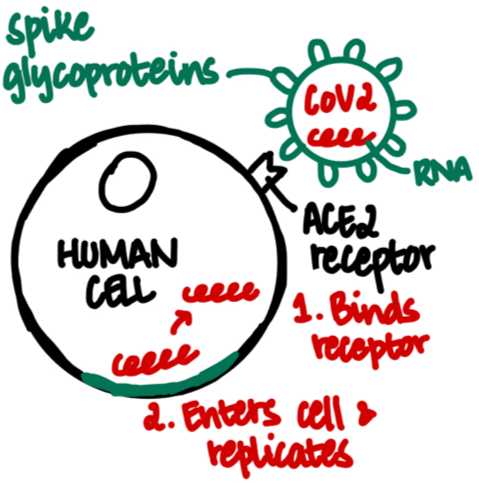
Image drawn by @nanduriac
In terms of possible targets for therapy, while studies are pending, we can consider the envelope as well as surface glycoproteins. The envelope has a crucial role in pathogenicity since it promotes viral assembly and release. There are two spike glycoproteins with 2 subunits on SARS-CoV-2 which can also be targeted. While the S1 subunit has high variability, the S2 subunit is highly conserved.
So what are potential target anti-viral options to inhibit an uncontrolled infection of the virus?
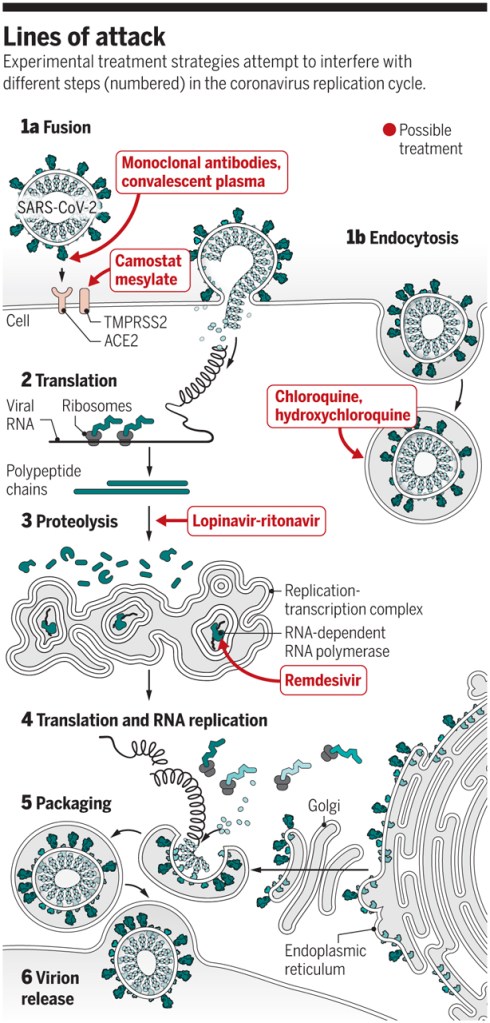
Let’s dive into a few of the above, focusing primarily on Hydroxychloroquine. We can also touch briefly on the discussion regarding steroids and IL-6 inhibitors.
Why all the hype with Hydroxychloroquine?
Hydroxychloroquine is an anti-malarial with anti-inflammatory effects that is presently used to alleviate symptoms in patients with rheumatologic disease. It differs from chloroquine by the presence of a hydroxyl group at the end of the side chain. It has fewer side effects, when compared with chloroquine, is rapidly absorbed through the gut, and is excreted renally.
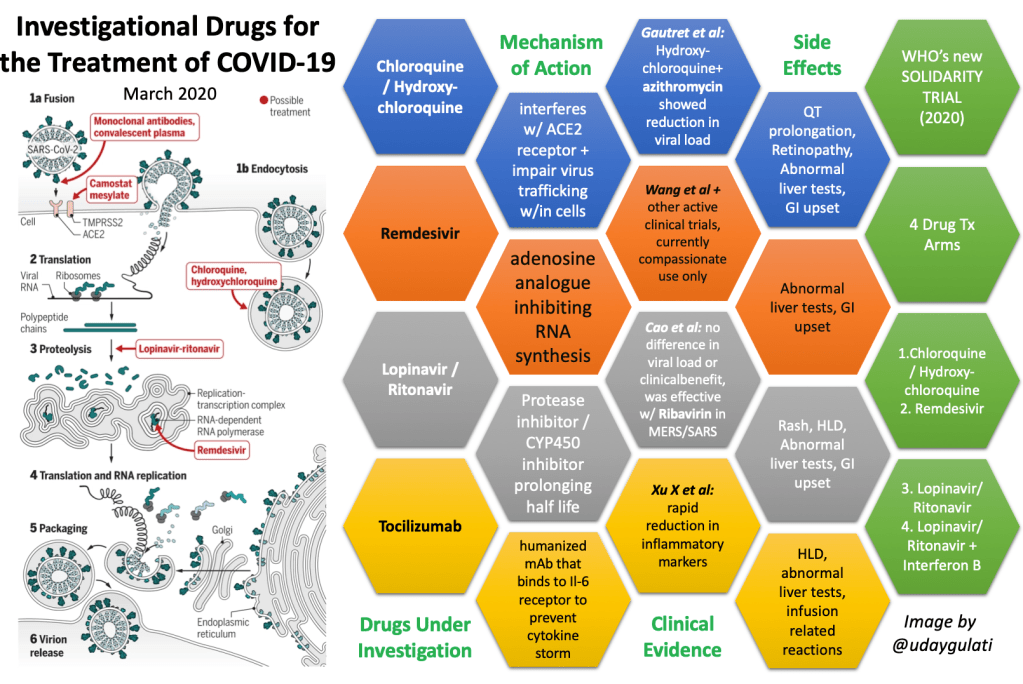
There are more than a dozen trials studying the efficacy of chloroquine or hydroxychloroquine in the treatment of COVID-19. While there are without a doubt plenty of limitations and biases amongst these studies, example: the popular Gautret et al. study (3/29/30), they do, to some extent, demonstrate the superiority of hydroxychloroquine compared to control treatment in shortening disease course by inhibiting exacerbation of existing pneumonia as well as promoting virus-negative conversion.
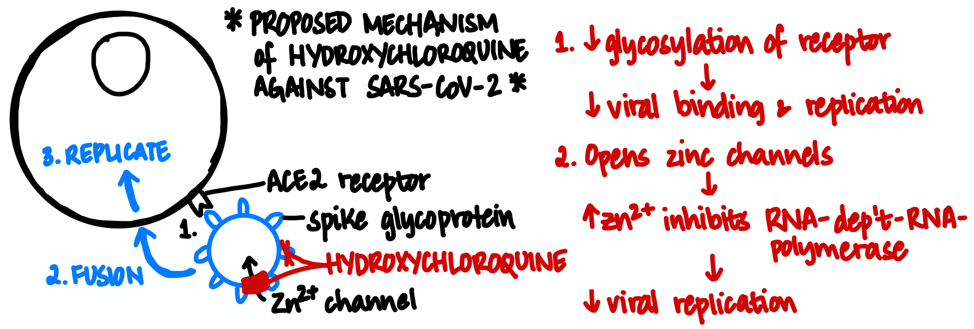
Image by @nanduriac
In vitro studies have shown that hydroxychloroquine has better activity against SARS-CoV-2 than chloroquine, exact length of treatment has varied but a loading dose of 400 mg twice daily is recommended followed by 200 mg twice daily for 4 days and up to 10 days.
The latest news: As of 3 AM EST on 03/30/2020, the FDA has issued emergency approval for the use of hydroxychloroquine and chloroquine in the treatment of SARS-CoV-2. While there is minimal evidence to support the efficacy of this treatment, this has likely been put into effect due to the rapid increase in cases and the desperate need for treatment. Millions of doses have been also been donated as there was a growing shortage of hydroxychloroquine, which does treat many patients with rheumatologic conditions. Clinical trials, like WHO’s SOLIDARITY trial are pending and definitive treatment has yet to be identified.
So you plan on initiating therapy? Before initiation of hydroxychloroquine, get a baseline ECG, renal function, liver function and complete blood count. Hydroxychloroquine can cause cardiac side effects and is contraindicated in patients with prolonged QT as well as conduction delay and cardiomyopathy. Daily ECGs can evaluate for new onset conduction delay as well as prolonged QT. Daily magnesium and potassium levels are important. While presence of renal dysfunction or hepatic dysfunction are relative contraindications, depending on severity, patient can still receive medications at reduced doses. Liver function tests must be obtained daily due to the hepatotoxicity. This medication can also cause numerous hematologic abnormalities such as aplastic anemia, leukopenia, thrombocytopenia, it is relatively contraindicated in G6PD deficient patient. It is contraindicated in pregnant females.
| Organ System | Monitoring | Side effects |
| HEENT | Baseline ocular testing and visual acuity | Irreversible retinopathy |
| Cardiovascular | ECG daily Mg > 2, K > 4 2D Echo, as needed | QT prolongation, worsened when combined with Azithromycin. Conduction abnormalities such as new BBB or AV delay. Cardiomyopathy |
| Renal | BUN, Cr Urine output | Reduce dose if presence of renal dysfunction as it is renally excreted. |
| Gastrointestinal | LFTs | Acute liver failure Nausea, vomiting, diarrhea |
| Hematologic | CBC | (Aplastic) anemia Leukopenia Thrombocytopenia |
| Endocrine | Blood glucose | Hypoglycemia > consider decreasing dose of anti-hyperglycemic if initiating medicine |
Why is it recommended to pair with azithromycin?
The same French study by Gautret et al. that showed “reduction of viral carriage” after 6 days of treatment was with Azithromycin and compared to patients not receiving Azithromycin. However, the combination of Azithromycin and Hydroxychloroquine has yet to be studied in a clinical trial. There is significant QT prolongation with the addition of azithromycin to Hydroxychloroquine.
Most patients presenting with COVID symptoms should be started on empiric therapy for community acquired pneumonia, especially as there is increased risk for secondary bacterial pneumonia co-infection. Consider following the IDSA guidelines for pneumonia coverage for the first 48 hours after presentation. Antibiotics can be discontinued if work up for bacterial pneumonia is negative, which should be in the differential and initial treatment plan for patients with non-specific respiratory symptoms.
What about Remdesivir?

Remdesivir is an antiviral drug that has shown to effectively inhibit RNA-dependent-RNA-polymerase, enzyme that allows viral RNA replication, of coronaviruses in vitro. There are currently three clinical trials to determine efficacy against SARS-CoV-2. Until 03/23/2020, the medication was available to the critically ill patients with COVID-19 for compassionate use.
What about Lopinavir/Ritonavir/Ribavirin?
Maybe. Cao et al. recently reported no reduction in viral load with lopinavir/ritonavir combination drug. However, there may be some promise with the triple agent. Lopinavir is a protease inhibitor whereas Ritonavir is a CYP450 inhibitor that prolongs the half-life of lopinavir. Ribavirin is a guanosine analog that inhibits viral RNA replication. It works in synergy with lopinavir. The combination of three medications has been shown to be efficacious against coronavirus but as yet, no promising results have been presented and the triple therapy regimen is not recommended.
What about IL-6 inhibitors?
In some patients, there are notable cytokine storms with increases in IL-6 and IL-10 prior to multi-organ failure. While hydroxychloroquine has immunomodulatory effects to decrease the production of cytokines, there is also consideration for anti-IL-6 medications.
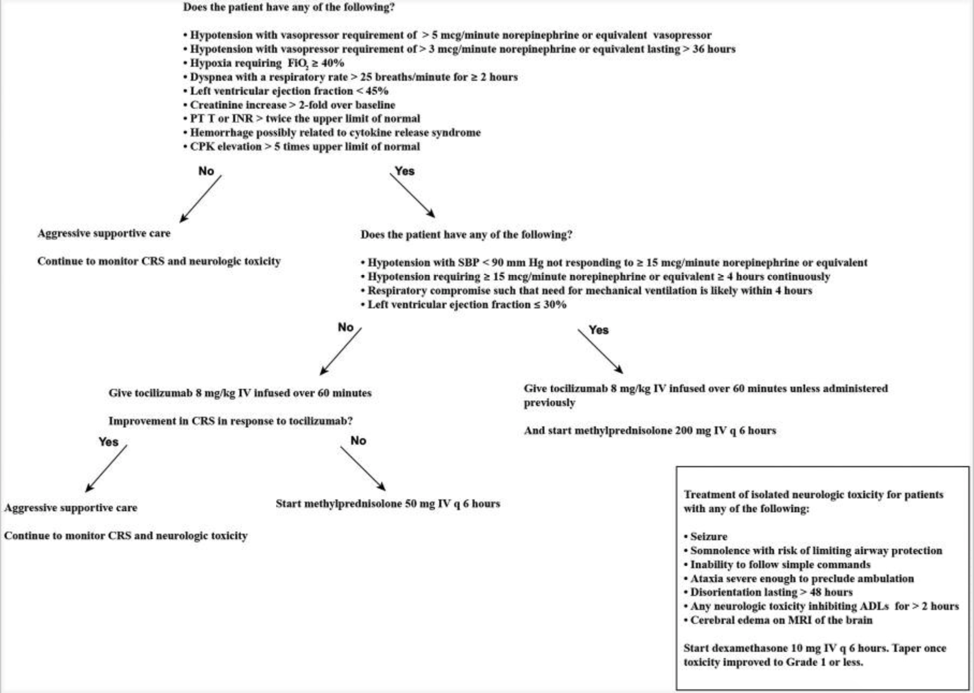
For patients with extensive lung injury and presenting with multi-organ failure with increased levels of IL-6 on testing, China’s protocol has recommended using tocilizumab. However, studies are not currently available for the use of anti-IL6 agents routinely. Most recently, Genentech’s COVACTA trial received FDA approval on 03/23/2020 to evaluate Actemra (Tocilizumab) in adult patients hospitalized with severe COVID-19 pneumonia compared to placebo. Also, on 03/18/2020, EUSA Pharma in Italy has initiated the SISCO study to evaluate the efficacy of Siltuximab in patients with serious respiratory complications.
Some side effects of IL-6 receptor antagonism are thrombocytopenia, neutropenia, upper or lower respiratory infections, possibility of neurologic side effects although poorly defined at present and liver dysfunction. The recommended dose of tocilizumab is 4-8 mg for 1 dose. If there are no side effects or lack of response, another dose can be given 12 hours later or IV steroids can be added to the treatment regimen.
Wait, steroids? For a viral infection?!
No! Certainly not for routine use for patients presenting with any viral illness such as influenza or coronavirus as it can increase viral shedding. In severe cases of acute lung injury, low dose steroids may be beneficial be helpful by decreasing systemic inflammation and cytokine release.
Villar et al.’s DEXA-ARDS trial noted reduced hospital length of stay in patients with bacterial pneumonia as well as decreased respiratory deterioration and lower ICU mortality in patients with acute lung injury from leukemia. So, there may be a benefit in using dexamethasone in very sick patients. Wu et al. recently studied the efficacy of methylprednisolone in ARDS patients and reported reduced mortality. This was a small study and further evaluation is required but in the very ill patients who are refractory to other treatment, it may be beneficial to consider steroids to mitigate the neutrophilia in these patients as well as the cytokine storm.
In summary…
- The initial recommendation for patients with respiratory symptoms with concern for COVID is to rule out any other underlying causes such as influenza, rhinovirus, RSV and treat for bacterial pneumonia, until work up is negative. Patients should remain on precautions until testing returns negative.
- Daily lab work is important. For patients who are worsening, thorough evaluation to identify any organ dysfunction is crucial.
- At present, there are no established antiviral therapies for COVID-19. The data we have are from small cohort studies with many clinical trials pending results.
- Anti-IL6 agents are essentially last course of therapy for patients who have multi-organ dysfunction and/or ARDS. Overall pathogenesis and treatment options are poorly understood at present. This is an evolving situation and the virus is being studied rigorously to identify the mechanism of action and how to effectively treat patients.
- The literature and recommendations will constantly change as more and more is published. The historic trial to really look forward to is WHO’s multinational SOLIDARITY Trial. Stay informed!
- On 03/30/2020, the FDA did issue an emergency approval for the use of hydroxychloroquine and chloroquine in the treatment of SARS-CoV-2. While there is minimal evidence to support the efficacy of this treatment, this has likely been put into effect due to the rapid increase in cases and the desperate need for treatment.
- The discussions regarding evidence-based management of respiratory distress and ARDS management of SARS-COV-2 are the topic of a whole other post, or few, and to be had with our ICU and pulmonary specialists. Stay Tuned!
Post reviewed and edited by @udaygulati
References:
Brudno JN, Kochenderfer JN. Recent advances in CAR T-cell toxicity: Mechanisms, manifestations and management. Blood Rev. 2019;34:45–55. doi:10.1016/j.blre.2018.11.002
Cao B, Wang Y, Wen D, et al. A Trial of Lopinavir-Ritonavir in Adults Hospitalized with Severe COVID-19. The New England Journal of Medicine. 2020. doi: 10.1056/NEJMoa2001282
Cascella M, Rajnik M, Cuomo A, et al. Features, Evaluation and Treatment Coronavirus (COVID-19) [Updated 2020 Mar 8]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK554776/
Devaux CA, Rolain, J, Colson, P, et al. New insights on the antiviral effects of chloroquine against coronavirus: what to expect for COVID-19? International Journal of Antimicrobial Agents. 2020. https://doi.org/10.1016/j.ijantimicag.2020.105938. Available from: https://www.sciencedirect.com/science/article/pii/S0924857920300881?via%3Dihub#bib0059
Fehr AR, Perlman S. Coronaviruses: an overview of their replication and pathogenesis. Methods Mol Biol. 2015;1282: 1–23. doi:10.1007/978-1-4939-2438-7_1
Gautret P, Lagier J, Parola P, et al. Hydroxychloroquine and azithromycin as a treatment of COVID‐19: results of an open‐label non‐randomized clinical trial. International Journal of Antimicrobial Agents – In Press 17 March 2020 – doi.org/10.1016/j.ijantimicag.2020.105949
Gordon CJ, Tchesnokov EP, Feng JY, et al. The antiviral compound remdesivir potently inhibits RNA-dependent RNA polymerase from Middle East respiratory syndrome coronavirus. Journal of Biological Chemistry. 2020. doi: 10.1074/jbc.AC120.013056
Plaquenil (Hydroxychloroquine): Uses, Dosage, Side Effects, Interactions, Warning. (2020, February 19). Retrieved from https://www.rxlist.com/plaquenil-drug.htm#warnings
Villar, J, Ferrando, C, Martinez, D, et al. Dexamethasone treatment for the acute respiratory distress syndrome: a multicenter, randomized controlled trial. The Lancet. 2020; 8(3): 267-276. doi.org/10.1016/S2213-2600(19)30417-5
Wang D, Hu B, Hu C, et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus–Infected Pneumonia in Wuhan, China. JAMA. 2020;323(11):1061–1069. doi:10.1001/jama.2020.1585
Wu C, Chen X, Cai Y, et al. Risk Factors Associated With Acute Respiratory Distress Syndrome and Death in Patients With Coronavirus Disease 2019 Pneumonia in Wuhan, China. JAMA Intern Med. Published online March 13, 2020. doi:10.1001/jamainternmed.2020.0994
Xue J, Moyer A, Peng B, et al. Chloroquine is a zinc ionophore. PLoS One. 2014;9(10):e109180. Published 2014 Oct 1. doi:10.1371/journal.pone.0109180
Xueting Y, Fei Y, Miao Z, et al. In Vitro Antiviral Activity and Projection of Optimized Dosing Design of Hydroxychloroquine for the Treatment of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2), Clinical Infectious Diseases, doi.org/10.1093/cid/ciaa237
