
A 23-year-old female w/ no significant PMHx presents with SOB and RLE pain. She describes it as sudden onset and pleuritic. She does not take any medications including hormonal birth control. She denies any recent surgical history. She is unaware of any family history of clotting or bleeding disorders. Aside from sinus tachycardia, her vitals are unremarkable and she remains hemodynamically stable. Her cardiopulmonary and GI exam are unremarkable. She has a positive Homan’s sign on her RLE. EKG shows sinus tachycardia. Aside from negative troponins, routine labs are unremarkable. Given obvious clinical suspicion, a CTA and RLE US were obtained that showed subsegmental pulmonary embolism and popliteal vein VTE w/o phlegmasia cerulea dolens. With minimal risk of bleeding, no significant past medical history and no concern for medication noncompliance, she is initiated on empiric anticoagulation with Eliquis. (see considerations of picking a therapeutic regiment).
Routine DVT/PE workup and treatment, right? Question is, why did she have a blood clot? Does she need a hypercoagulable work? What entails a hypercoagulable workout?

Why determine the cause of a VTE?
The benefits of determining the cause of a VTE include
- Determining duration of therapy, example someone with a hypercoagulable disorder would be considered for lifetime VTE prophylaxis versus somoene with a provoked cause such as surgery only needs 3 months
- Identification of inherited thrombophilia may result in avoidance of precipitating meds such as hormonal contraception due to increased risk
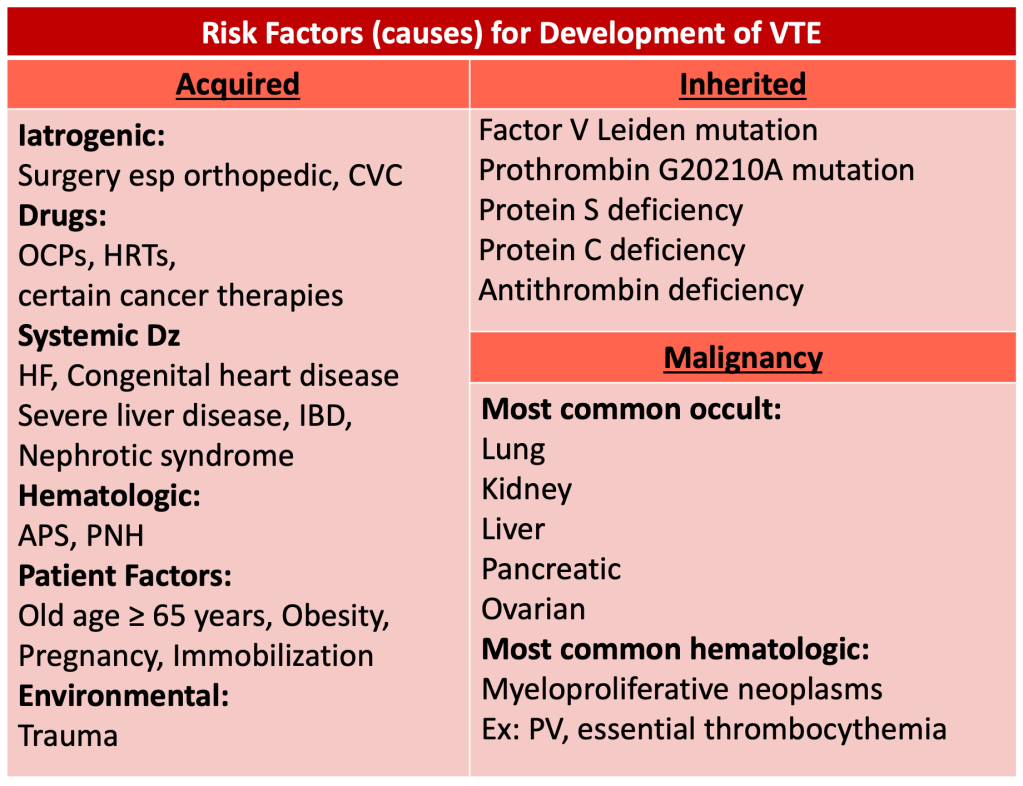
What are the risk factors for development of having a blood clot?

Unfortunately, at our level, saying Virchow’s triad is as good as saying something that would make you see a doctor.
But there are identifiable risk factors that we can look for.
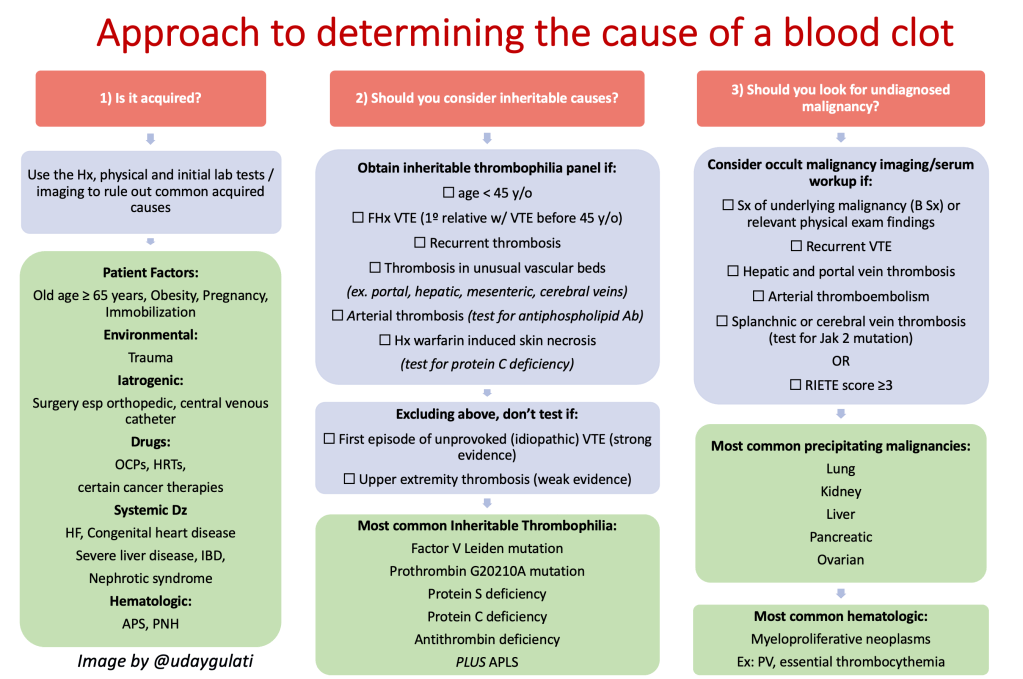
How can you narrow your DDx?
Understandably, it would be unreasonable to test everyone for all of the causes of a blood clot every time someone presents with a VTE. It’s a game of numbers. We can try and narrow down our differentials based on information easily obtainable by the history, physical exam and initial lab tests and imaging.
Try this cheat sheet:
History:
Ask about
- Recent surgeries or trauma, recent hospitalizations, pregnancy or immobility
- PMHx of thromboembolism or significant prothrombotic disorders ex. SLE, myeloproliferative neoplasm, nephrotic syndrome, IBD, etc.
- Use of precipitating medications: OCP, HRT, consider drugs that induce lupus anticoagulants or antiphospholipid antibodies such as hydralazine or procainamide
- if applicable, OB history: Recurrent fetal loss? i.e. APS; second or third trimester fetal loss? i.e. Inherited thrombophilia
- FHx of venous thrombosis especially in 1 or more first-degree relatives? I.e. hereditary thrombophilia
- ROS for constitutional symptoms appoint with underlying malignancy I.e. B symptoms
Physical exam
- findings that points towards malignancy ex. lymphadenopathy, breast masses, ascites, hepatomegaly, edema
Initial Lab Tests
In regards to very nonspecific initial lab tests to point you in the right direction:
| Elevated hematocrit/platelet count +/- splenomegaly | myeloproliferative neoplasms ex. PV, essential thrombocythemia |
| Anemia/leukopenia/thrombocytopenia | PNH |
| Thrombocytopenia on heparin therapy | HIT |
| Schistocytes or RBC fragmentation | DIC TTP HUS |
| Leukoerythroblastic nucleated red blood cells | Bone marrow involvement by tumor |
| Unexplained prolonged aPTT | lupus anticoagulant/APLS |
| Positive Hemoccult | GI malignancy |
| Multiple thrombosis or thromboses in unusual organs ex. mesenteric, hepatic, portal, splenic, renal, cerebral veins | Malignancy myeloproliferative neoplasms inheritable thrombophilia nephrotic syndrome PNH |
| Arterial thrombosis | APLS myeloproliferative disorders nephrotic syndrome malignancy |
Anything that pops up on this initial information collection should be further explored. However, once you’ve confidently ruled out any of the acquired causes, is it time to look for inherited or malignant causes?
Which patients do you select for work-up of inherited disorders?
The hypercoagulable work-up is a set of specific tests looking for the inherited hypercoagulable disorders discussed above. Specifically, if you are trying to create an order set for inherited thrombophilia, the list includes:
- Protein S
- Protein C
- Antithrombin
- Factor V Leiden
- Prothrombin gene mutation
For a subset of patients, you should also include the work-up for Antiphospholipid Syndrome (APLS) which includes
- Screening test: Anticardiolipin and lupus anticoagulant
- Confirmatory test: Hexagonal phase Anti-prothrombin antibody
You are not going to order these tests on everyone because it usually does not alter therapeutic or prophylactic anticoagulation management and based on multiple studies, has not been associates with improved mortality outcomes.
We can consider obtaining these tests based on the following criteria:
- younger than 45 years old
- a strong family history of VTE ie a first-degree relative with documented VT before the age of 45
- recurrent thrombosis
- thrombosis in unusual vascular beds example portal, hepatic, mesenteric, cerebral veins
- arterial thrombosis (only looking for antiphospholipid antibodies)
- history of warfarin induced skin necrosis (only looking for protein C deficiency)
Who do you not test for inheritable thrombophilia?
Based on pretty convincing evidence, there are patients who you should definitely NOT obtain a hypercoagulable work up for. Excluding those listed above, you can avoid testing in those with:
- first episode of unprovoked (idiopathic) VTE (strong evidence)
- upper extremity thrombosis (weak evidence)
This is because in these patients testing for hereditary thrombophilia does not affect clinical management. There is no mortality benefit. It does not reduce risk of recurrence. Despite the risk of not identifying a inheritable hypercoagulable disorder (present in ~42% patients of first unprovoked VTEs) in unprovoked VTEs, it is the unprovoked nature of the event rather than the underlying disorder that determines the risk of recurrence and duration of anticoagulation. Similarly, despite the higher incidence of inheritable thrombophilia in UE thrombosis, identifying the disorder did not affect the risk of future recurrence. However, other studies have shown conflicting data so one is definitely justified in obtaining a thrombophilia workup.
Which patients do you select to look for malignancy?
AKA on whom will you obtain extensive tests to look for occult cancer? For most patients, this is not necessary. This was made pretty convincing in the landmark SOME Trial. There was no clinical benefit in doing so given that the prevalence of occult cancer was low among patients with a first unprovoked venous thromboembolism.
However, some can be risk stratified to be at higher risk of having a precipitating malignancy. The most common precipitating malignancies being ovarian, pancreatic, liver, kidney, and lung cancer. An extensive work up to look for these precipitating malignancies could include but may not be limited to:
- Chest, abdominal, pelvic CT scan
- Tumor markers example CEA, alpha-fetoprotein, CA 19–9, CEA 125, PSA
- Mammography
- Upper and lower GI tract evaluation
PET combined with CT(almost never recommended based on previous trials showing no benefit)
Outside of routine initial labs and XR imaging, this additional testing is only considered in patients thought to have a high risk of having malignancy. The obvious benefit would only be earlier identification of a cancer as multiple meta-analyses and retrospective studies have shown limited prevention of cancer related death.
The high risk population is to consider testing would be patients w/:
- symptoms of underlying malignancy (B symptoms) or physical exam findings discussed above
- recurrent VTE
- hepatic and portal vein thrombosis
- arterial thromboembolism
- splanchnic or cerebral vein thrombosis (specifically get the Jak 2 mutation to look for underlying myeloproliferative disorder)
PEARL: Alternatively, consider using the RIETE score to identify patients that are high risk.

It’s simple, one point each for:
- male gender
- age > 70 years
- chronic lung disease
- anemia
- elevated platelet count
- prior VTE
- recent surgery
Based on the MVTEP study, cancer was diagnosed in 11.8% of patients determined to be high risk (score ≥ 3) versus only 3.6% in those determined to be low risk (score ≤ 2). Check it out!
In summary:
- Look for causes of a provoked DVT starting with the history, physical, initial routine labs and diagnostic imaging. Use the cheat sheet and table above
- Once you’ve confidently ruled out risk factors for acquired causes, consider a hypercoagulable work-up for the 5 inherited disorders and APLS in patients w/ the following criteria:
- younger than 45 years old
- a strong family history of VTE ie a first-degree relative with documented VT before the age of 45
- Recurrent thrombosis
- Thrombosis in unusual vascular beds example portal, hepatic, mesenteric, cerebral veins
- Arterial thrombosis (only looking for antiphospholipid antibodies)
- History of warfarin induced skin necrosis (only looking for protein C deficiency)
- Look for occult malignancy with extensive imaging and certain tumor markers and those with:
- symptoms of underlying malignancy (B symptoms) or physical exam findings discussed above
- Recurrent VTE
- Hepatic and portal vein thrombosis
- Arterial thromboembolism
- Splanchnic vein thrombosis or cerebral vein thrombosis (specifically get the Jak 2 mutation to look for underlying myeloproliferative disorder)
- Always engage in a risk/benefit discussion with your patients before obtaining these additional test for inherited and malignant causes, understanding that it only serves a limited purpose and usually does not alter mortality or management
References:
Carrier M, Lazo-Langer A, Shivakumar S, et al. Screening for occult malignancy in unprovoked venous thromboembolism. N Engl J Med. 2015;373:697-704
Baglin T, Gray E, Greaves M, Hunt BJ, Keeling D, Machin S, Mackie I, Makris M, Nokes T, Perry D, Tait RC, Walker I, Watson H, British Committee for Standards in Haematology Clinical guidelines for testing for heritable thrombophilia. Br J Haematol. 2010;149(2):209.
Middeldorp S, van Hylckama Vlieg. A Does thrombophilia testing help in the clinical management of patients? Br J Haematol. 2008;143(3):321.
Rivaroxaban vs warfarin in high-risk patients with antiphospholipid syndrome. Blood. 2018 Sep 27;132(13):1365-1371. doi: 10.1182/blood-2018-04-848333. Epub 2018 Jul 12.)
Post reviewed and edited by @udaygulati

One thought on “When do you perform a hypercoagulable workup?”