
You are evaluating a 55-year-old male with significant past medical history of non-insulin diabetes, recently treated Lyme disease, and immigrant from India 25 years prior who is presenting with a 2-week duration of persistent fevers, chills, malaise and myalgias. After a week inpatient with an overall negative microbiology and rheumatologic work-up, his fevers are persistent despite broad-spectrum antibiotics. Can you call this a fever of unknown origin (FUO)? If so, how do you want to continue your management and workup?
Even with modern diagnostic tools and advanced therapeutic possibilities, FUO is on the rise and remains one of the unresolved challenges in medicine. When diagnosed, it requires an extensive differential to test for.
This will be the first of a two-part post. The first is an interesting tale of the evolving definition and epidemiology of FUO. The second will be a clinical approach as to what to do once you have made the diagnosis including the additional work-up to try and figure out the underlying cause.
How is FUO defined?
This has changed quite a bit over the last 50 years so first, a bit of history. This was initially defined by Petersdorf & Beeson in 1961 as:
- Temp. > 38.3 C (101 F)
- Duration of fever > 3 weeks
- Failure to reach a diagnosis despite 1 week of inpatient investigation
This was then further classified in 1991 by Durack & Street into the following entities based on an understanding that immunocompromised patients would have a notably different spectrum of underlying illnesses and approaches to management:
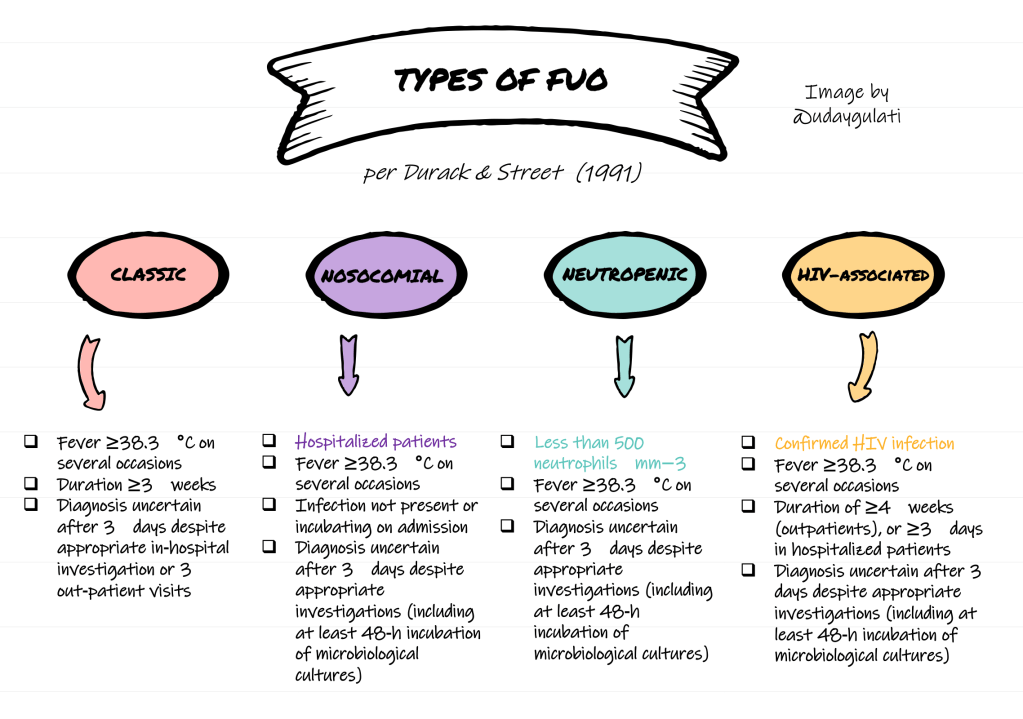
It makes sense: consider that in those with neutropenic fevers we start empiric antibiotics but in those with classic FUO, empiric antibiotics is not recommended. Here we focus on the immunocompetent adult outpatient. Plus, immunocompromised patients were excluded from a lot of the studies that analyzed diagnostic protocols for classic FUO.
In regards to classic FUO, Durack and Street defined a required duration of investigation: 3 outpatient or 3 days in-hospital. This was based primarily on the time needed for classical cultures and skin tests to become and be reported as positives. However, with eventual advancements in outpatient imaging and diagnostic utilities, Knockaert et al. proposed a revised definition in 2003 that was generally well received and has been used in most studies since. They defined FUO as:
- Fever > 38.3 C (101 F) on at least 2 occasions
- Duration of fever > 3 weeks
- Without an established etiology despite an “appropriate intelligent” investigation (see below)
In simpler terms, consider FUO if:
“prolonged febrile illness of at least 3 weeks duration that does not have established etiology despite an ‘intelligent’ work-up.”
Knockaert et al. (2003)
What does an “intelligent” work-up entail?
In order to conclude that the patient has FUO, the following should have been performed and determined to be unremarkable:

After that, any further evaluation will directed by abnormalities detected on the evaluation above.
Conclusion
- The definition of ‘Fever of Unknown Origin’ (FUO) has changed often since the first popular published criteria in 1961.
- This includes 4 different entitites by Durack & Street (1991) based on an understanding that immunocompromised patients have a different spectrum of underlying illnesses and approach to management:
- classic FUO
- nosocomial FUO
- neutropenic FUO
- HIV-associated FUO
- A recent, commonly supported definition by Knockaert et al. (2003) defines FUO as:
- Fever > 38.3 C (101 F) on at least 2 occasions
- Duration of fever > 3 weeks
- Without an established etiology despite an “appropriate intelligent” investigation (see above)
Well, your work doesn’t stop there. Now what about trying to diagnose the underling cause? What about management in the interim? Stay tuned for part II of this post!
References
Knockaert DC, Vanderschueren S, Blockmans D. Fever of unknown origin in adults: 40 years on. J Intern Med. 2003;253(3):263‐275. doi:10.1046/j.1365-2796.2003.01120.x
Bleeker-Rovers CP, Vos FJ, de Kleijn EM, et al. A prospective multicenter study on fever of unknown origin: the yield of a structured diagnostic protocol. Medicine (Baltimore). 2007;86(1):26‐38. doi:10.1097/MD.0b013e31802fe858
Kouijzer IJE, Mulders-Manders CM, Bleeker-Rovers CP, Oyen WJG. Fever of Unknown Origin: the Value of FDG-PET/CT. Semin Nucl Med. 2018;48(2):100‐107. doi:10.1053/j.semnuclmed.2017.11.004
Keidar Z, Gurman-Balbir A, Gaitini D, Israel O. Fever of unknown origin: the role of 18F-FDG PET/CT. J Nucl Med. 2008;49(12):1980‐1985. doi:10.2967/jnumed.108.054692
Post reviewed and edited by @larrybuck2.

One thought on “How do you define FUO?”