
So you have determined that your patient meets criteria for a fever of unknown origin (FUO). How? See Part 1 of this post. Now how do you further work up FUO and rule out a broad list of differentials? What about antipyretic, anti-inflammatory or antibiotic management in the interim? Let’s dive in.
Recall the “intelligent” work-up?
Recall, that first, in order to be able to ‘diagnose’ a fever as one of ‘unknown origin’, you have to obtain an initial “intelligent” work-up.

From this initial evaluation, you can start exploring any abnormalities.
What are your differentials?
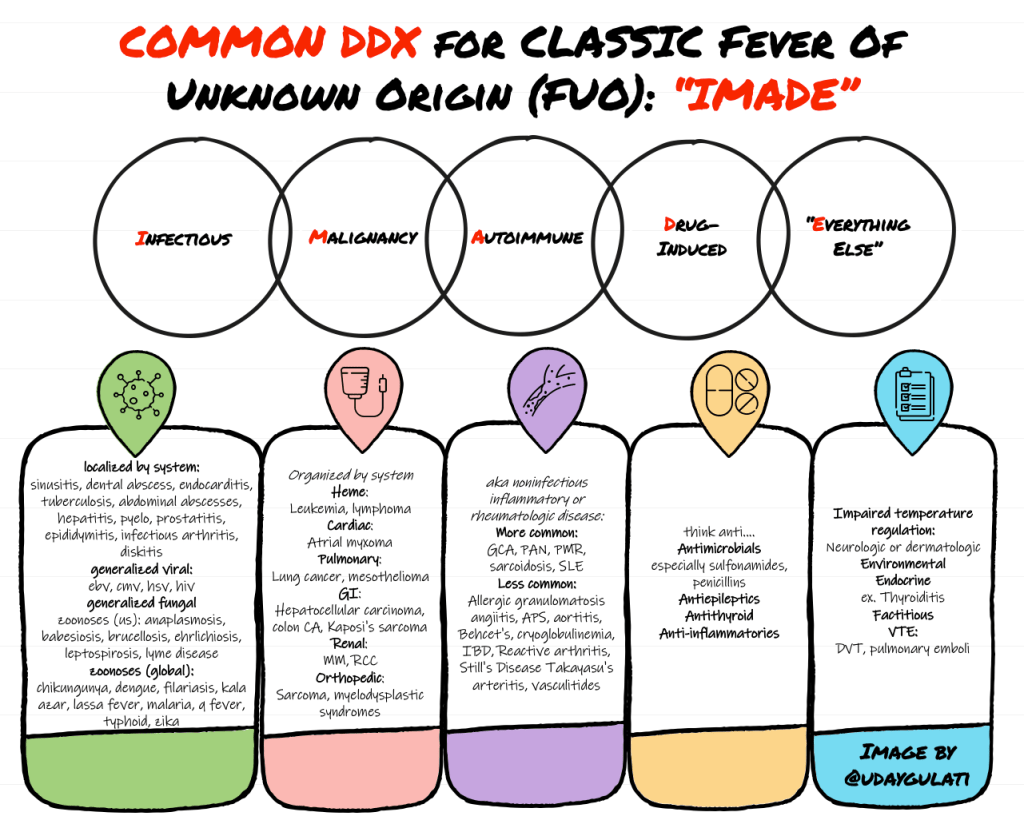
When attempting to determine the underlying cause of the now-diagnosed FUO, try the inflammatory mnemonic “iMADE”:
- Infection
- Malignancy
- Autoimmune (Rheumatologic)
- Drug-induced
- Everything else
It might be impossible to have a fully inclusive list so included below are the most common is in each category:
How do you approach this “additional” investigation?
The following can be considered for further evaluation based on any abnormalities on the initial ‘intelligent’ work up, including the history and physical exam:
- HIV immunoassay and viral load
- CMV‐IgM and EBV serology in case of an abnormal CBC differential
- Endocrine work-up
- Echocardiography in case of a cardiac murmur or risk factors
- CT chest/abd/pelvis
- Nuclear medicine studies: FDG-PET scans, Gallium scan, and Indium scans
In regards to the actual utility of all the tests above, keep in mind:
- based on prior trials most of the imaging tests have a false positive rate similar to the rate of a helpful result
- acute phase reactants such as ESR and CRP are extremely nonspecific. In a prior JAMA study of 263 patients with an ESR >100, 50% had malignancy and 25% had an infection or an inflammatory disease. Other ideologies that can also raise the ESR significantly include drug hypersensitivity reactions, thrombophlebitis and renal disease. On the contrary, a normal ESR or CRP, with a few exceptions, usually suggest that a significant inflammatory process is absent.
- CT scans are essentially being used on all patients due to their ability to find
- small nodules which could suggest fungal/mycobacterial/nocardial infections or malignancies
- Hilar mediastinal adenopathy which could prompt a biopsy by mediastinoscopy to diagnose lymphoma, histoplasmosis or sarcoidosis
- abdominal lymphadenopathies which could suggest lymphoma or granulomatous processes
- an MRI, while usually more sensitive, only needs to be considered when ruling out certain diagnoses like a spinal epidural abscess
- while exploratory laparotomies used to be used to evaluate FUO, they have been replaced almost completely by CT scanning
What about nuclear medicine scanning?
Nuclear medicine testing is generally reserved for patients in whom initial evaluation including abdominal and chest CT remains negative. While gallium–67 and indium–111 labeled leukocyte scans are highly sensitive by virtue of scanning the entire body, they are extremely nonspecific unless used to localize a concerning site identified on initial CT imaging. Alone, prior studies have found the rate of a helpful result similar to the rate of false positives.
On the contrary, F–fluorodeoxyglucose positive emission tomography (FDG–PET) scans, seem to have an increasing appeal as part of diagnostic protocols to evaluate FUO. In 3 trials that evaluated the use of FDG-PET scans as part of a diagnostic protocol to evaluate FUO, these scans were determined to be clinically helpful 33% of the time in a 2006 study, 66% of the time in a 2015 retrospective analysis, and 56.7% in a 2018 prospective study. These scans are extremely sensitive in identifying anatomical sites of inflammation or malignancy.
So when should you order the FDG-PET scan?
This is commonly debated in the literature and warrants a literature review of its own. In our review, there is a trend towards “earlier the better”. In one literature review by Kouijzer et al., the authors go far enough to make the conclusion that FDG-PET/CT should become a routine procedure in the workup of FUO when diagnostic clues are absent and should be performed when fever is present or within 1 week in case of an elevated CRP. Keep in mind that with a lot of the FUO work up being done outpatient, this will likely be ordered during an inpatient workup.
What about the other ‘more specific’ testing?
A high index of suspicion for a specific etiology should come with an inclination to obtain the respective specific testing. As with any invasive testing, you must ask, what is the positive predictive value (PPV) of this test before opening them to the risks of such procedure?
- CNS symptoms? Get an LP and imaging of head/spine
- Returning traveler? Refer to your ‘Fever in a Returning Traveler’ algorithm
- Travel to Midwest or Southeast? Test for the respective fungal pathogens based on geography
- Travel to malaria–endemic regions? Thick and thin smear
- Signs of VTE? Venous duplex or CTA
- Liver lesions? Liver biopsy
- Lymphadenopathy? Lymph node biopsy
- Clinical findings of PAN? Temporal artery biopsy
- Lab values supporting hematologic malignancies? Bone marrow biopsy
What about empiric treatment?
Empiric treatment, also referred to as “therapeutic trials”, stems from a common inclination to “do something” prior to establishing a diagnosis. Should you start steroids when you suspect an inflammatory process? Should you start antibiotics if you suspect an infectious cause?
While there is no guideline-based answer, the expert recommendation has generally been that if they are clinically stable, the answer is no as they can interfere with diagnostic evaluation. For example, consider:
- that the diagnostic yield of repeat blood cultures is reduced after starting antibiotics.
- that certain antibiotics being started for a suspected but unconfirmed infection may suppress the ability to detect a difficult-to-isolate organism causing a different type of infection
- that even with antibiotics, certain infections take a while for the fever to resolve so it would be difficult to determine duration of empiric antibiotics based on just a fever
- that a trial of glucocorticoids will decrease diagnostic yield of biopsies for steroid-responsive diseases
- that a trial of glucocorticoids prior to thoroughly evaluating for infection can be harmful to the patient
What about antipyretics?
First, ensure there is no hyperpyrexia (extraordinarily high fevers >41.5°C common in severe infections or CNS hemorrhages) or hyperthermia. If simply a fever, then yes. If the patient is uncomfortable they help with headaches, myalgias, arthralgias and fatigue. In older adults, they may also help with delirium. However, maintain caution with unnecessary use of acetaminophen or NSAIDs as they may obscure symptoms and signs of certain diseases during the diagnostic evaluation process.
What about undiagnosed FUOs?
Despite advances in diagnostic testing and imaging, serial studies have shown that while the fraction of undiagnosed FUO’s dropped from over 75% in 1930s to less than 10% in the 1950s, it increased notably up to ~51% in the 2000s (based on a systemic review in 2003).
How?
- Consider that with advancing diagnostics and the adjustments in criteria to diagnose FUO, the initial ‘intelligent’ work up provides earlier insight into the cause of persistent fevers thereby decreasing the incidence of ‘true’ FUOs. This would have resulted in an increased incidence in undiagnosed FUO’s.
- Also consider that the increased use of empiric antibiotics, anti-inflammatories or other medications could be masking the underlying cause or be precipitating drug fevers. This has likely played a role in the evolving distribution of underlying causes seen above.
Nevertheless, mortality outcomes seem to be reassuring. While the outcome depends on the underlying diagnosis, a few studies showed that most adults who remained undiagnosed on discharge had a favorable prognosis.
Conclusion
- While there are no set guidelines on how to approach FUO due to variations in definitions and proposed diagnostic algorithms that still require further investigation, we came up with the following (once again, not a tested algorithm):

- Avoid empiric treatment with antibiotics or anti-inflammatories as they affect diagnostic yield unless clinically unstable
- Assuming there is no hyperpyrexia or hyperthermia at play, allow symptomatic treatment of fever with antipyretics or anti-inflammatories once determined there is no diagnostic benefit of allowing the fever to persist.
- No guideline-published diagnostic algorithms are currently recommended but order specific tests based on high PPV
- While the fraction of FUO’s without an underlying cause has increased, the mortality
- outcomes of those with an undiagnosed cause remains favorable
References
Knockaert DC, Vanderschueren S, Blockmans D. Fever of unknown origin in adults: 40 years on. J Intern Med. 2003;253(3):263‐275. doi:10.1046/j.1365-2796.2003.01120.x
Bleeker-Rovers CP, Vos FJ, de Kleijn EM, et al. A prospective multicenter study on fever of unknown origin: the yield of a structured diagnostic protocol. Medicine (Baltimore). 2007;86(1):26‐38. doi:10.1097/MD.0b013e31802fe858
Kouijzer IJE, Mulders-Manders CM, Bleeker-Rovers CP, Oyen WJG. Fever of Unknown Origin: the Value of FDG-PET/CT. Semin Nucl Med. 2018;48(2):100‐107. doi:10.1053/j.semnuclmed.2017.11.004
Keidar Z, Gurman-Balbir A, Gaitini D, Israel O. Fever of unknown origin: the role of 18F-FDG PET/CT. J Nucl Med. 2008;49(12):1980‐1985. doi:10.2967/jnumed.108.054692
Post reviewed and edited by @larrybuck2.
