
An 81-year-old male with significant past medical history of CAD s/p single-vessel CABG, aortic stenosis s/p TAVR, atrial fibrillation on Coumadin presented to the ED after a syncopal episode. He described “blacking out” during ambulation without seizure-like activity. In the ED, he was found to be in sinus bradycardia with a heart rate in the 40s. He is admitted and the question you ask yourself as part of your initial assessment is “Does this patient require a permanent pacemaker (PPM)?”

Artificial cardiac pacemakers were developed to address symptomatic bradyarrhythmias, i.e. to maintain an adequate heart rate when the heart’s natural pacemaker isn’t fast enough to maintain adequate cardiac output or because of a threatening block in the heart’s electrical conduction. They do so by delivering electrical impulses to the heart muscle chambers, thereby replacing or regulating the heart’s electrical conduction system. That is as simple as it gets in terms of mechanism, explaining the pacing methods and types would require a post of its own. The following specifically focuses on indications for a permanent pacemaker as per recent cardiology guidelines. Unfortunately, these guidelines published in 2018 together by the American College of Cardiology (ACC), American Heart Association (AHA) and Heart Rhythm Society (HRS) provide a broad, detailed list of reasons with various ‘indications classes’ that, in all honesty, can be overwhelming to remember (see table below). Here we’ll attempt to break it down.
What are the general considerations towards PPM placement?
Per my review, there are 5 general considerations to keep in mind when determining the need for PPM placement for either symptomatic bradycardia or a bradyarrhythmia.

Being able to keep these 5 considerations in mind should help you elucidate organize most indications for a PPM. Let’s explore each one.
What are the classes of PPM indications?
As defined by the ACC/AHA/HRS guidelines, indication for pacemakers can be divided into 3 classes:

Due to notable ambiguity for indication for PPM placement, these classes have been applied to the most common indications of PPM listed above (point 4).
The goal of this post is to then simplify class I and II indications for these common indications in a manner easy to reference.
What are the symptoms associated with a bradyarrhythmia?
Primarily applicable to sinus node dysfunctions (SNDs) and acquired atrioventricular blocks (AVBs), these guidelines delineate the level, or strength, of indication for PPM based on being able to associate certain symptoms with a bradyarrhythmia. These symptoms generally include:
- Dizziness, lightheadedness
- Syncope
- Fatigue
- Poor exercise tolerance
However, ascertaining a direct connection between these symptoms and a bradyarrhythmia can be tricky: it largely depends on a solid history and being able to document the cardiac rhythm when symptomatic – via ECG or ambulatory monitoring (think external monitors or implantable loop recorders). For example, for a sinus node dysfunction, classes are based on symptoms and being able to associate those symptoms with the sinus bradycardia:

Therefore:
- establishing this connection increases the likelihood of benefit from PPM versus
- not being able to establish this connection decreases the changes of benefit from a PPM
Keep in mind, per the guidelines, there is no definitive threshold for heart rate that dictates an absolute indication for PPM placement. Rhythms that would fall under this classification of SNDs include:
- Sinus pauses (>3s)
- sinus bradycardia (<50bpm)
- sinus node arrest (no evidence of SN depolarization)
- ectopic atrial bradycardia (non-sinus)
- sinoatrial exit block (blocked conduction beating SN and atrial tissue, evidenced by group beating and sinus pauses)
- tachy-brady
- chronotropic incompetence (failure to attain 85% of expected HR during exercise)
- Isorhythmic dissociation (atrial rate slower than ventricular rate)
Where is the location of the conduction abnormality?
The first three of the underlying causes that warrant PPM are a conduction abnormality that can be located above the AV node, at the AV node, or below the AV node.
Arrhythmias caused by conduction issues originating below the AV node, i.e. the His-Purkinje system, are more likely to worsen than those within the AV node; thus rhythms pointing towards the former location will benefit from PPM placement than the latter.
The following can help determine the location:

Based on that concept, the guidelines recommend the following level of indications for acquired AV blocks:

Therefore, likely via ECG:
- establishing conduction abnormality below the AV node increases the likelihood of benefit from PPM versus
- establishing conduction abnormality at the AV node decreases the changes of benefit from a PPM
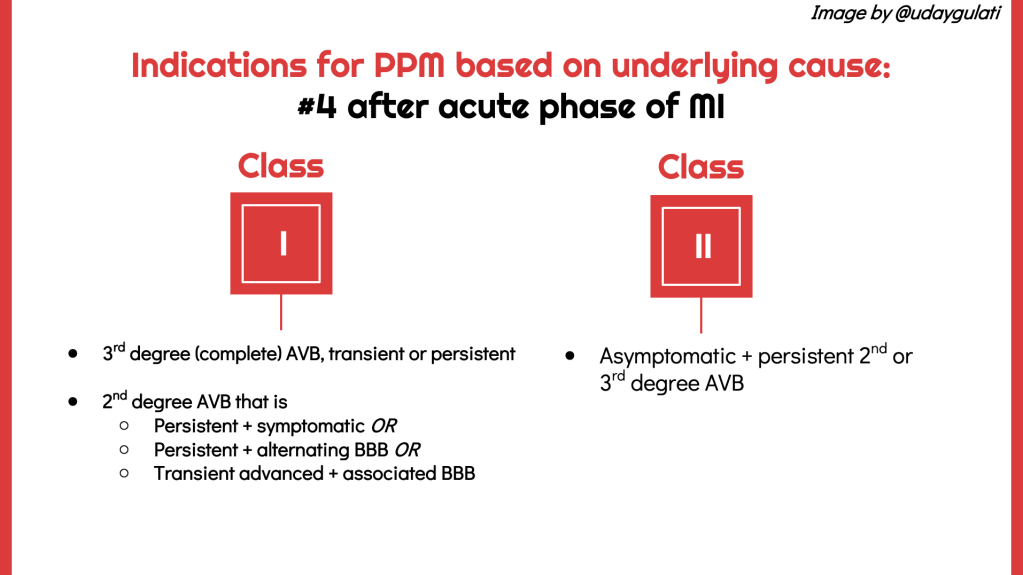
What is the underlying condition?
As mentioned above, the guidelines divide indications for PPM based on 10 “underlying conditions” to explain conduction issues. The first 5 are the most common, including #4 which points to acquired AV blocks after an MI and #5 neurogenic syncope usually due to a hypersensitive carotid sinus. We’ve discussed #1 (SND) and #2 (AVB), the following are the class I or class II recommendations for the remaining conduction abnormalities.







What about pacing for reversible causes?
While most of the above causes are due to intrinsic congenital or acquired conduction disease, a number of extrinsic precipitants cause reversible bradyarrhythmia. These include:
- Medications (e.g., beta blockers, non-dihydropyridine calcium channel blockers, antiarrhythmic medications [e.g., sotalol, amiodarone])
- Toxic, metabolic, and electrolyte disturbances (e.g., hyperkalemia, digoxin toxicity)
- Acute myocardial ischemia or infarction
- Cardiac trauma (e.g., post-operative, blunt chest trauma, indwelling pulmonary artery catheters)
- Infectious etiology (e.g., Lyme disease)
- Sleep apnea
- Subacute bacterial endocarditis (e.g. an aortic valve abscess damaging the His-Purkinje system)
If symptomatic, management of these reversible causes can be approached with temporary cardiac pacing until it resolves or long-term therapy can be initiated. Temporary cardiac pacing, usually via transvenous endocardial leads or transcutaneous leads in an emergency, will re-establish circulatory integrity and hemodynamics due to the slow heart rate. If due to one of the acute and reversible causes listed above, the bradycardia will usually not require permanent pacing and would fall under “class III” evidence to support NOT getting a permanent pacemaker. The obvious caveat is that if the underlying etiology continues to cause a symptomatic bradyarrhythmia, then it will fall under a class I or class II indication for a PPM. For example, if the underlying cause of a symptomatic SND is a medication for which there is no alternative, the patient would have a class I indication for a PPM.
Other class III conditions where pacing is not indicated include:
- Syncope of undetermined etiology: extensive testing including ambulatory monitoring, neurogenic or electrophysiologic testing needs to be done to hone in on an underlying cause prior to considering a pacemaker because permanent pacing may not alleviate the symptoms since no correlation has been confirmed
- Asymptomatic sinus bradycardia, sinoatrial block, sinus arrest, AV block that is first degree or second degree Mobitz I
- Asymptomatic bradycardia during sleep
- Asymptomatic cardioinhibitory response to carotid sinus stimulation (i.e. produces a slower heart rate but no syncopal episodes)
- Long QT syndrome or torsades de pointes due to reversible causes.
In Summary:
- Permanent pacemakers deliver electrical impulses to the heart muscle chambers to maintain an adequate heart rate when the heart’s natural pacemaker isn’t fast enough to maintain adequate cardiac output or because of a threatening rhythm in the heart’s electrical conduction.
- Per the ACC/AHA/HRS guidelines, specific indications are broad and detailed and divided into 3 classes, or level, of indication based on evidence of likely benefit.
- Primarily for SNDs, those with a clear association between the bradyarrhythmia and symptoms (dizziness, lightheadedness, syncope, exercises intolerance) are more likely to benefit from a pacemaker than those without.
- Primarily for AVBs, establishing conduction abnormality via ECG below the AV node increases the likelihood of benefit from PPM versus at the AV node.
- Further considerations are broken down by underlying conditions that would predispose a patient to symptomatic or life threatening arrhythmias that include chronic bifascicular blocks, neurocardiogenic response (ex. Hypersensitive carotid), post MI or cardiac transplant, HoCM, congenital heart disease and severe systolic HF.
- Consider reversible extrinsic causes of the bradyarrhythmia, most commonly medications, as that would be a contraindication to receiving a PPM.
Post reviewed by @nanduriac
References
Kusumoto FM, Schoenfeld MH, Barrett CN, Edgerton JR,Ellenbogen KA, Gold MR, Goldschlager NF, Hamilton RM, Joglar JA, Kim RJ, Lee R, Marine JE, McLeod CJ, Oken KR, Patton KK, Pellegrini CN, Selzman KA,Thompson A, Varosy PD. 2018 ACC/AHA/HRS guideline on the evaluation and management of patients with bradycardia and cardiac conduction delay: areport of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. J AmColl Cardiol 2019;74:e51-156
Dalia T, Amr BS. Pacemaker Indications. [Updated 2020 Feb 11]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK507823/
https://www.ahajournals.org/doi/10.1161/CIR.0000000000000628
